[icon name=”circle-exclamation” prefix=”fas”] This section of the website represents the historical record of a legacy programme which is no longer managed by TPHC, as of mid 2025.

The Community Led Prevention Team
(Formally Personalised Care)
In response to the NHS Long Term Plan (2019), the Health and Care Vision for London (2019), and the Mayor’s Health Inequalities Strategy (2018), a London-wide personalisation programme was established in 2019 as an evolution to what was previously London’s pro-active care programme.
Working in partnership with NHSE London, ICBs, GLA, OHID, Local Councils, PCNs and VCSE, the programme provided a dedicated regional transformation function to support London’s systems to embed, expand and maximise the impact of Social Prescribing on reducing health inequalities.
We worked alongside ICBs, borough-based teams and primary care, secondary care and community services, helping build the infrastructure to make this possible.
Our purpose
Our vision was for every Londoner to experience Personalised Care, where people are actively involved and connected to activities, groups, and services in their community that meet the practical, social and emotional needs that affect their health and wellbeing.
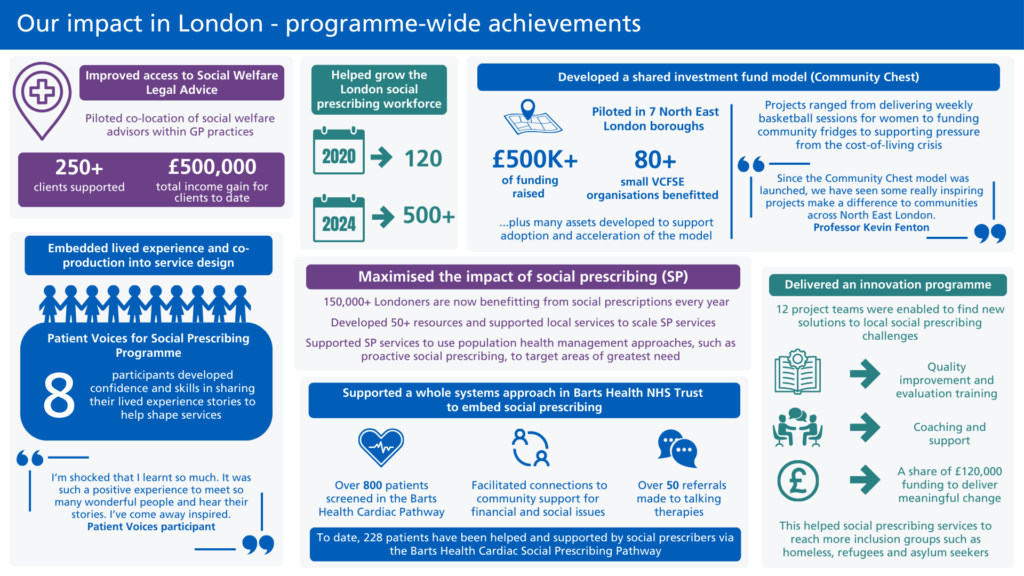
We supported over 500 social prescribing link workers, health and wellbeing coaches and care coordinators, based in London’s primary care networks.
These roles enable almost half a million Londoners to access personalised care and connections to local community and VCSE groups to address their non-clinical needs.

Our mission was to ensure these personalised care roles, and other community-led preventative services, are thriving.
This in turn supported London’s health and care systems to develop more proactive, preventative and community centred approaches to improve the health and wellbeing of those most impacted by health inequity.
Our core programme
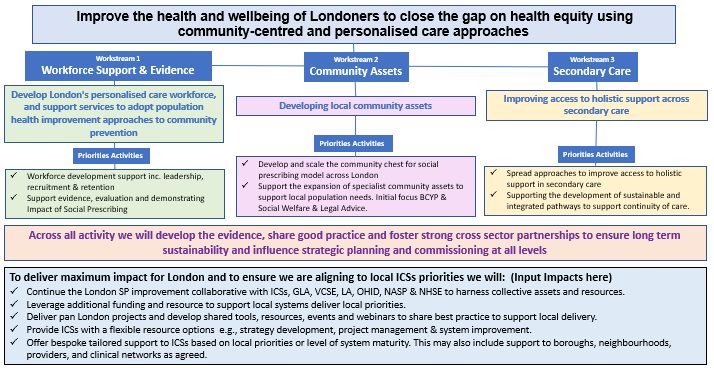
From 2023/24 the programme widened its scope beyond supporting the expansion of Social Prescribing to supporting wider community led approaches with the following ambition:
Supporting London’s health and care systems to develop more proactive, preventative and community centred approaches to improve the health and wellbeing of those most impacted by health inequity.
(At this point, the programme transitioned from Personalised Care to Community Led Prevention)
This was delivered through three work areas:
- Workforce Support & Evidence: Develop London’s personalised care workforce, and support services to adopt population health improvement approaches to community prevention
- Community Centred approaches: Develop local community assets and Improve access to specific support in the community which address the wider social and structural determinants of health
- Secondary Care: Improving access to holistic support across secondary care
Our 2023/24 work plan:
The impact of our programme
Programme transition in March 2025
The programme ran between April 2019 and March 2025. From September 2024, we initiated a transition phase in which our focus was to embed our work into sustainable structures including NHS England and ICBs.
To do this, we worked alongside ICB to co-produce plans and help develop the infrastructure for transformation of social prescribing and community led services. Read more about our transition work here.
Our Workstreams
Historic workstreams
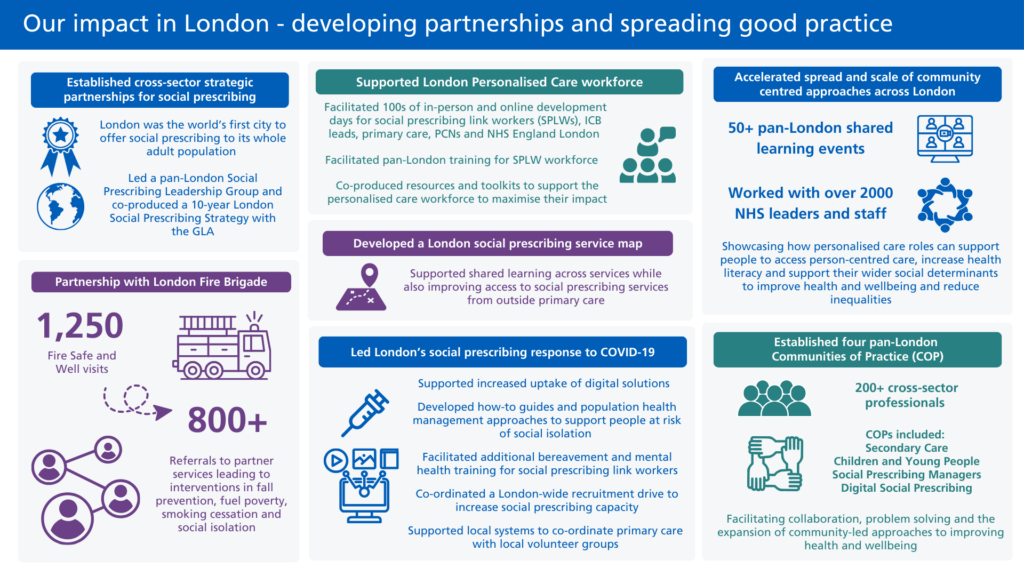
Holding roles funded by NHS England, we worked directly with the personalised care workforce and their managers across London, convening roles together in peer support meetings and organising webinars to help them problem solve, learn and network. We fed back challenges to NHS England to shape national guidance and outputs.
We helped support the spread, scale-up and sustainability of CYP social prescribing across London. We worked directly with local areas to support delivery of CYP social prescribing pilots, for example in NEL and NCL. In addition, we convened a pan-London Community of Practice to provide a peer support opportunity for CYP social prescribing link workers and gathered case study examples to share learnings from across London and wider.
Read more about the Children and Young People (CYP) Social Prescribing workstream here.
Core workstreams
We set up once for London projects to develop the infrastructure around support for the personalised care roles and their managers. This helped tackle shared challenges such as a lack of local peer support, and understanding among PCNs on how the roles should connect to existing teams. In addition, with worked with ICBs to tackle local challenges, developing workshops and tailored support.
Read more about the Workforce and System support workstream here.
We brought together a diverse range of system partners and people working on the frontline to share best practice and challenges to demonstrating social prescribing impact. We co-produced outputs to help tackle the challenges and help local services evaluate their impact. We worked alongside NASP and NHSE to shape national work to evidence social prescribing.
We supported the development of personalised care initiatives in secondary and acute care pathways in London. By sharing case studies and learning, we developed the evidence base and understanding of funding models, referral pathways, cohorts and evaluation methods. We provided direct support and convened a community of practice to scale new approaches to personalised care in specialisms including cardiac, cardiac rehab, HIV and more.
Read more about the Proactive / preventative models in health care: Secondary care workstream here.
We support London’s ICBs to increase provision of and better integrate social welfare legal advice within healthcare and other settings. We convened pan-London groups to continue building momentum and support the culture shift on SWLA within healthcare. In addition, we developed resources, built the evidence base and communicated the impact of integrating social welfare legal advice.
The Patient Voices for Social Prescribing programme was a pilot programme to empower and amplify patient voices of social prescribing in London. It gave the opportunity for people with lived experience to share their experiences, build skills and confidence in telling their story and explore opportunities to help improve social prescribing services in London.
Read more about the Proactive / preventative models in health care: Patient Voices workstream here.