Service specification for delivering mental health care to people experiencing homelessness
Introduction
The purpose of this document is to provide guidance and recommendations on Mental Health provision for people experiencing homelessness.
For the purposes of this document, the recommendations are for services working with people who are currently experiencing Rough Sleeping, and so do not include wider definitions of homelessness. This is a decision reached by the consensus of the TPHC led MH and homelessness steering group.
This consensus was reached as most teams in London specialising in this work have that remit. However, we would like to stress that any interventions for people experiencing Rough Sleeping with a Mental Health need should include a continuation of specialist support after they are housed. In areas where this cannot be supplied, there need to be effective pathways and handovers to mainstream services, who may need to flex to accommodate the needs of this cohort.
The Steering Group acknowledges the challenges in what we are recommending in the current climate and welcome your feedback and views.
The steering group recognises that people experiencing wider forms of homelessness (TA, sofa surfing, supported accommodation, CAS3 accommodation etc) also face barriers when needing to access statutory MH services, and acknowledge the need for further guidance and recommendations for this cohort.
Authors
Rae Clarke (Co-occurring Conditions Project Officer, TPHC)
Fran Busby
Alison Bearn
Context
- There is an increasing awareness of the need for a bespoke approach to service provision for inclusion health populations including those experiencing homelessness (NHS Long term plan on Health Inequalities- HiQiP, Core20PLUS5, improving access and outcomes). Evidence shows that individuals with lengthy histories of rough sleeping can often have significant health and social care needs that are not met by mainstream approaches to care. The Kerslake Commission outlined the need for integrated local strategies for Wellbeing Boards/ ICS and LAs to address these inequalities. The publication of the NICE Guidelines for homelessness in March 2022 provided clarity as to how such services should be commissioned and delivered to achieve successful outcomes. Recent guidance from ADASS following the Everyone In Initiative also outlines best practice in statutory services working effectively with people experiencing homelessness and third sector partners.
- CHAIN/ GLA figures for 2023/24 show that 11,993 people slept rough in London 19% on 2022/23.
- In Q1 of 2024 4,223 people slept out, this is 29% more than Q1 of 2023. (CHAIN/GLA reporting).
- Last years CHAIN report (GLA/ CHAIN, 2024) demonstrates that 48% of rough sleepers have mental ill health and 30% co-occurring substance use and mental ill health. Local data from London mental health teams (see appendix A) demonstrates the efficacy of a specialist approach to supporting people experiencing homelessness with such needs.
- 10,053 people were seen tough sleeping by outreach workers in London during 2022/23. The most frequently reported support need amongst people seen rough sleeping was mental health, with 51% of those assessed during the period having a need in this area (CHAIN)
- Transformations in Health and Care and Homeless Health London Mental Health clinical leadership group are comprised of a wide variety of professionals working in the field from both statutory and third sectors, as well as people with lived experience. This specification has been developed following a Pan London scoping exercise and aims to set out best practice in this area.
Vision
- We believe that all people experiencing homelessness in a local authority/ commissioning area are residents of that area and deserve the same access to care as those with a settled address. However, evidence demonstrates that to achieve the same access and outcomes for individuals requires a specific service design.
- Guidance and local evidence demonstrates that that such teams need to deliver care via outreach methods that are relationally focused, multi-disciplinary and integrated between health and social care, with small caseloads, allowing them to work intensively and flexibly across transitions and to collaborate with third sector services.
- Unless such teams are explicitly commissioned and designed with these approaches in mind they will struggle to effectively identify, engage and achieve recovery goals with those they support.
Case study 1
The following case studies provide an example of the approach and work in a specialist MDT for people experiencing homelessness: access to care is improved by specialist outreach teams with all services under one roof.
Shelly is a 35-year-old Somali woman with a history of early trauma. She lost her flat and son after an episode of post-natal illness, was not seen by mainstream services and ended up street homeless. She was evicted repeatedly from hostels and TA for assaulting staff in what appeared to be highly dysregulated states but was seen as having substance misuse issues. She was unable to engage with any mental health care or assessment. The team care coordinator started working with Shelly when she moved into an Assessment Centre and built a positive, confiding relationship based on understanding her early experiences, tolerating resistance to contact and offering consistent care. This led to a more robust assessment and eventually an inpatient admission under the MHA. She was diagnosed with Bipolar Affective illness, treated and moved into specialist hostel. She sees her MDT worker regularly, continues medication, is seeing her sister again and is soon to step down to low support housing.
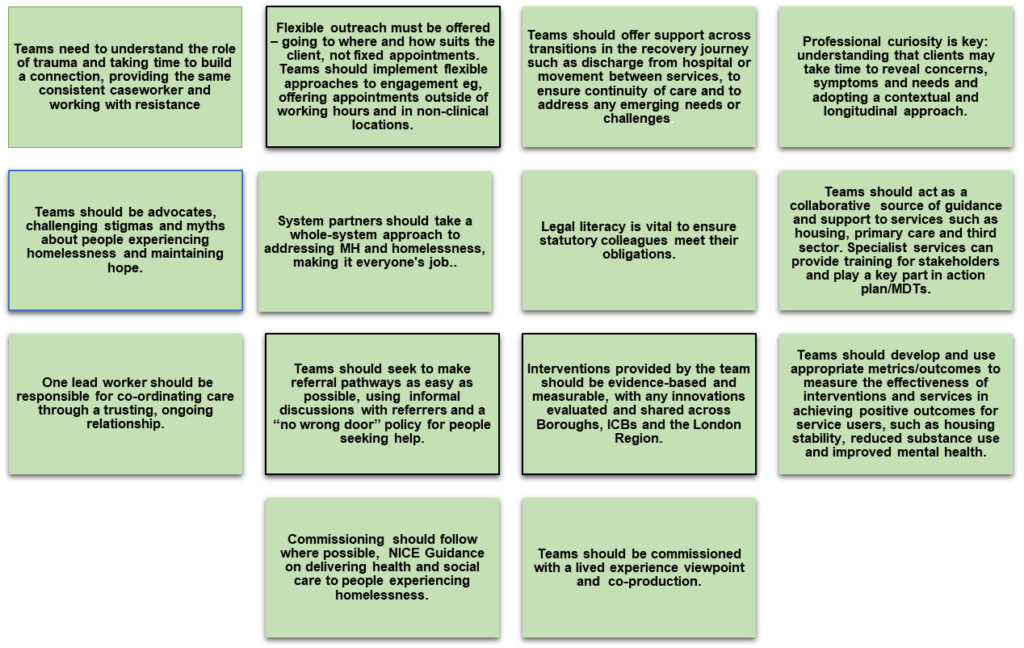
Core values/approaches
Evidence Base
- Stop the Scandal (St Mungo’s report) outlines significant gaps in services for people experiencing homelessness and mental ill health (2016)
- In 2020 NHSE awarded 7 national areas 5-year funding to deliver specialist mental health care for people experiencing homelessness. These projects were aimed at delivering learning and outcomes across 5 domains: access to mental health and substance use care, access to physical healthcare, reduction in use of emergency care including A&E/ ambulance call outs and reduction in contact with the criminal justice system.
- All of these outcomes sought to deliver not only improvements in health status and quality of life but also cost savings to the wider health and social care system and to community well-being. One of these pilots was established in LB Lambeth and awarded to the South London and Maudsley START Homeless Outreach Teams to run a team providing dual diagnosis care into hostels. Initial findings at mid project report showed significant recovery outcomes (see appendix A).
- https://www.london.gov.uk/media/102896/download – RAMHP NEL Outcomes
- NICE Guidance directs us to commission and deliver services via the statutory integrated MDT:
- The Dame Carol Black report recommends adopting trauma informed commissioning at LA level and ICBs adhere to NICE guidelines https://ukhsa.blog.gov.uk/2021/07/13/dame-carol-blacks-independent-review-of-drugs-prevention-treatment-and-recovery/
- Clients benefit from co-produced services where they have agency and are able to feedback around their care needs https://cpb-eu-w2.wpmucdn.com/blogs.ucl.ac.uk/dist/c/605/files/2021/02/Co-Pro-Stories-Short-Final.pdf
- The Health and Care Act 2022 is designed to enable a more joined up, collaborative system with feedback and input from service users https://www.england.nhs.uk/long-read/working-in-partnership-with-people-and-communities-statutory-guidance/
- ‘an ideal service would have a team of people that worked with you to plan your journey through treatment together. It would have your drug worker…, a psychologist supporting you with your mental health, a housing worker planning to get you into suitable accommodation, and a peer mentor who could help get you involved in things (like) fun activities’ – NEGC Member (lived experience)
Area specific needs
- Individual ICBs should assess the needs of people experiencing homelessness in each LA including demographics and diversity, health and social care needs, numbers rough sleeping and in hostel provision.
- Provision may be shared within an NHS trust (as in the cases of the RAMHP teams), individually within LA areas, or on a wider area basis. Recommendations are not prescriptive and each area needs to take it’s position within wider systems into account when deciding how to best work in this area.
- Effective formal service level agreements with Primary Care, Adult Social Care, Criminal Justice, Substance Use services, third sector and community mental health care are essential to create a recovery network.
- Additional training can be offered by specialist teams to partner agencies to builds capacity and expertise with this cohort.
- Handover and referrals onto other services need to be managed in a holistic and trauma informed way
- Referral processes need to be well planned and adapted to the area’s needs.
- The MDT will require agreed step-down pathways that local systems adhere to avoid flow issues in the service.
- Each borough, trust or area in which a team is based should agree a clear definition of homelessness & target group for their homelessness M.H outreach services – we recognise that these definitions and levels of need will differ in each area.
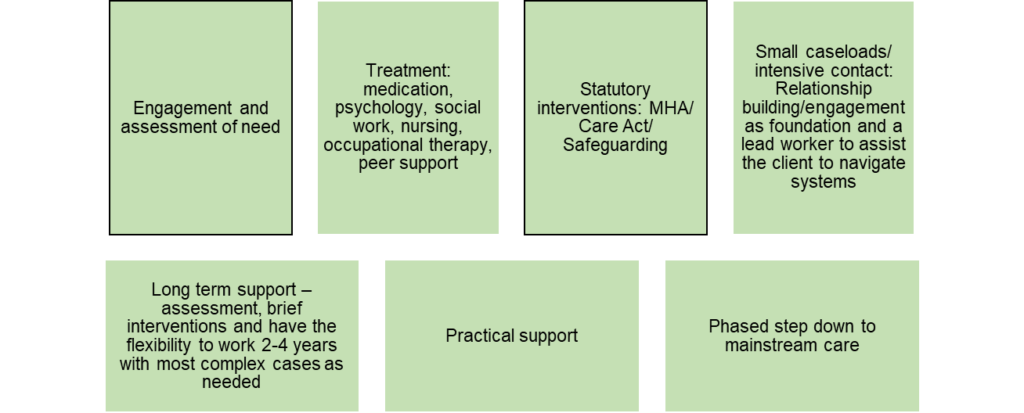
Key interventions
Where services are not commissioned to deliver ongoing interventions themselves, these interventions need to be transferred to mainstream services with robust referral routes, integrated pathways and comprehensive handovers of care.
Additional recommendations
- Service design needs to be done in a consultative manner from the beginning with embedded co-production.
- MDTs should create roles for people with lived experience and embed them across service delivery
- MDT service delivery techniques outlined in this document and accompanying guidance should be used as shared learning for wider Trust and LA networks to work more effectively with this cohort.
- Specialist MDTs will be involved with upskilling other teams to maintain the pathway into mainstream care.
- The MDT will aim to work with clients across transitions in their recovery to sustain progress.
Case Study 2
Nicky is a 45-year-old Spanish man who is a long term alcohol user and has a diagnosis of post traumatic stress. He has been street homeless for many years due to lack of benefits. He has repeated crisis presentations. He was referred by his hostel in a state of profound self-neglect: he was incontinent and his room full of hoarded rubbish. For weeks he just shouted at his social worker: eventually persistence paid off, he was supported to see the hostel GP and clean his room and see the addictions psychiatrist.
His social worker built a trusting relationship, built on understanding his early experiences and hands on support and work around harm minimisation and after 6 months Nicky went to detox and rehab and was resettled out of London.
Levels of offer
- The group recognises that different boroughs and areas have a range of needs assessment and that a variety of levels of provision would be appropriate.
- For boroughs or trust areas with minimal rough sleeping figures, NICE recommends that commissioners consider a specialist, homelessness “champion” role, based in mainstream care.
- Based on the current scoping exercise and guidance, we would expect each commissioning lead to ensure one of the following offers:
- Basic provision For a rough sleeping population of 30 or less
- 0.2 WTE of psychiatry, 1.0 WTE team leader, 2x 1.0 WTE Case workers (ideally a mix of social work and nursing)
- Full provision For a rough sleeping population of 30 -50 including some hostel provision
- 0.4 WTE of psychiatry, 1.0 WTE team leader, 3 x 1.0 WTE Case workers (ideally a mix of social work and nursing, occupational therapy), 0.4 WTE psychology
- Extended provision: To open up the service to clients with co-occurring conditions 50-60 cases
- 0.6 WTE of psychiatry, 1.0 WTE team leader, 4 x 1.0 WTE Case workers (ideally a mix of social work and nursing, occupational therapy) , 0.4 WTE psychology, 1.0 WTE Peer support, 1.0 WTE general nursing for physical health, 1.0 WTE Nurse prescriber for OST, 0.4 WTE General practice doctor
Appendix A
Outcome data from START Homeless Outreach Teams:
NHSE MH/ HOMELESSNESS PILOT PROJECT 2020-2025:
- 89% of caseload sustained accommodation
- 21 % of caseload had positive move-on (affected by availability)
- 55% of clients were engaged in positive physical health interventions.
- 55% of the caseload accessed substance use treatment (Tier 3 and 4) through support of the care coordinators.
- 88% of the caseload accessed mental health treatment (medication, psychosocial support, psychiatry).
- 32% % reduction in contacts with the Criminal Justice system each quarter.
- 26% reduction of physical health emergencies across the caseload over the whole timeframe (LAS call out, A&E attendance).
- 58 % reduction of mental health emergency contacts on average, per quarter (A&E attendance, S136, LAS call out).
OHID ROUGH SLEEPING DRUG AND ALCOHOL GRANT 2022-2025:
- 67% of caseload sustained accommodation and/or had positive move-on.
- 63% of clients were engaged in positive physical health interventions throughout the lifespan of the project.
- 48% of the caseload received psychological input from the team clinical psychologist.
- 72% of the caseload accessed substance use treatment through support of the care coordinators.
- 86% of the caseload accessed mental health treatment (medication, psychosocial support, psychiatry).
- There was a 16% reduction in contacts with the Criminal justice system from October 2021 to March 2024
- A 49% reduction of physical health emergencies (A&E) from October 2021 to March 2024
- A 61% reduction of mental health emergency contacts from October 21-March 24
Appendix B
References:
- Care and Support and Homelessness: Top tips on the role of Adult Social care (LGA and ADASS,2022)
- Integrated health and social care for people experiencing homelessness, NICE guideline (NG214, 2022)