Mpox Guidance for Homeless and Inclusion Health Settings
The following page provides information to help manage the health needs of inclusion health populations in London impacted by the mpox virus.
Please find background information on mpox as well as some guidance for managing suspected cases in a long- or short-term shared-living setting such as a hostel.
This page will be updated periodically to align with the most recent guidance, but for the latest information on mpox cases in England, see GOV.UK.
Latest guidance
Mpox in the UK
The UKHSA (UK Health Security Agency) has identified multiple confirmed cases of mpox in the UK.
It’s usually a mild illness that settles on its own, but it can sometimes become more serious. The UKHSA will contact people who have been in contact with a known case and may offer a vaccination.
The strain found in the UK is the ‘West African clade’. This usually causes a less severe illness and the risk of serious complications (including death) from an infection is around 1%.
What are the symptoms?
- The symptoms of mpox begin 5-21 days (average 6-16 days) after being exposed to the virus
- Usually, the first signs are a high fever, muscle and joint aches, enlarged lymph glands and a severe headache
- 1 to 5 days after initial symptoms a rash appears. The rash often starts on the genitals or face before spreading to other parts of the body
- The rash changes and goes through different stages before finally forming a scab which later falls off leaving healthy skin underneath. Once the final scab has fallen off, the individual is no longer infectious

How can mpox be treated?
Mpox is usually mild, and most people will recover within a few weeks without any treatment.
You should call NHS 111 or a sexual health centre immediately if you or a client have a rash with blisters. Self-isolate and avoid close contact with other people until you’ve been told what to do. Treatments such as ibuprofen and paracetamol can help with the fever and aches. Sometimes people become more unwell and need to be admitted to hospital. Urgent medical advice (call 111) if they develop any of these symptoms:
- Confusion
- Severe pain around lesions (e.g., if it prevents urination or defaecation)
- A worsening chest infection
- The surface of the eye is affected
- If there are over 100 lesions on the skin
Some people are at increased risk of complications for mpox. So, it’s important to avoid contact with these groups:
- Pregnant women
- Children under 12
- Immunosuppressed people
How do you catch mpox?
Mpox does not spread easily between people, but person-to-person spread may occur through:
- Direct contact with the skin lesions or scabs
- Contact with clothing or linens (such as bedding or towels) that have been used by an infected person
- Breathing in droplets from the coughing or sneezing of someone who has a mpox rash
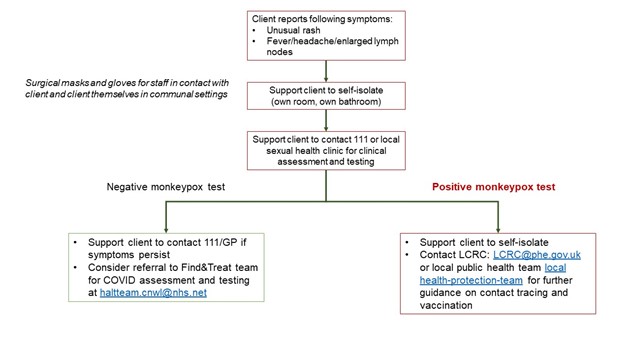
What to do if a resident/client has symptoms?
- Contact 111 or local sexual health service to access assessment and testing for mpox (highlight if you think they are clinically vulnerable and/or immunocompromised)
- Support them to self-isolate (own room, own bathroom), find more information on supporting self-isolation of residents/clients here
- Mopox can only be confirmed by testing using swabs
- Symptomatic resident should avoid contact with people at increased risk of complications (as above)
- Avoid skin to skin contact with others
- Don’t share plates, cutlery, bedding, towels and other linen
- Plates and cutlery can be washed in diluted bleach (check instructions on bottle). Wash clothes and bedding on a hot wash
- The main risk for transmission would be from direct contact with skin lesions or through contact with a patient’s clothing or linens that have been in contact with the lesions
- Therefore, staff should avoid touching skin lesions with bare hands, wear
disposable gloves and observe strict hand hygiene - Surgical masks can reduce droplet/airborne transmission
What to do if the resident/client is confirmed as having mpox?
- If the client tests positive, they need to continue to isolate until the last scab comes off
- Find more information on supporting self-isolation of residents/clients here
- If they have to travel, a surgical mask and covering lesions, reduces risk of transmission
What to do if they are contacts of a confirmed case of mpox (within the last 3 weeks)?
- The UKHSA local Health Protection Teams are contacting all confirmed cases to help prevent transmission to others
- Contact local health-protection-team or lcrc@phe.gov.uk
- Contacts should self-isolate at home for 21 days. Follow the same advice on travel, plates, bedding etc.
- Links to further information about cleaning of areas/surfaces if confirmed case Mpox_Guidance__cleaning_decontamination.pdf
Further information can be found here
[icon name=”circle-exclamation” prefix=”fas”] This section of the website represents the historical record of a legacy programme which is no longer managed by TPHC, as of mid 2025.