This page is no longer being updated from 31st March 2025.
Please visit Evelina London’s website here to view information and how to get involved.
Options to read this public consultation document
You can either read the consultation document below, or:
We want your views
We want your views on proposals for the future location of very specialist cancer treatment services for children who live in south London and much of south east England.
The consultation is led by NHS England London and South East regions. The consultation runs from 26 September to 18 December 2023.

Introduction
by former UK national cancer director, Professor Sir Mike Richards CBE MD FRCP; FRCR (Hon); FRCPath (Hon); FRCSE (Hon)
In 2019, I was asked by the Chief Executive of NHS England to carry out an independent review to help with a draft service specification for children’s cancer services. The central issue was whether or not it should be a requirement for Principal (main) Treatment Centres for children’s cancer, planned and funded by NHS England, to be on the same site as a level 3 children’s intensive care unit (which can give life support to the most seriously ill children).
I read all the documents from the public consultation on the draft specification. I read previous reports and guidance. I sought views from parents, charities, service leaders and clinical staff providing services, academics and clinical experts across the country. I visited key sites in south London (The Royal Marsden Hospital, St George’s Hospital, Evelina London Children’s Hospital and King’s College Hospital). I went to Great Ormond Street Hospital and University College Hospital in north London and one specialist children’s hospital outside London.
My conclusion was that all Principal Treatment Centres must be on the same site as a children’s intensive care unit and other specialist children’s services. This was supported by the vast majority of those I spoke to and by previous reports. You can read my report here.
The current Principal Treatment Centre for children with cancer living in south London and much of south east England is split across two sites. The majority of specialist care for children with cancer happens at The Royal Marsden in Sutton. Children’s intensive care, most children’s cancer surgery and other specialist children’s services are at St George’s in Tooting.
This means that most of the specialist cancer doctors at The Royal Marsden who are in charge of patients’ care are on a different site from the sickest patients, who are at St George’s. I commend the staff who work tirelessly to manage the risks of this and recognise that a Royal Marsden consultant is at St George’s every day. But the current arrangements should not continue longer than necessary.
Moving specialist cancer services to a site with a children’s intensive care unit would help us achieve the very best outcomes for children with cancer. It will become even more important for children’s care in future years, as the complexity of treatments for children’s cancers increases.
My report was published in January 2020 and was accepted in full by the Board of NHS England. Then came the pandemic. There is now no reason for further delay. Changes to bring specialist children’s cancer services on to the same site as children’s intensive care must proceed.
Professor Sir Mike Richards

Foreword
When a child is ill with cancer it’s hugely stressful for them, their parents and families. As the NHS England leaders for London and South East regions, we want children to get the best care in the best way.
To provide the very best care for children with cancer, specialist children’s cancer services currently provided by The Royal Marsden NHS Foundation Trust need to move to be on the same site as a children’s intensive care unit.
This consultation will help to answer the question “Where should the proposed future children’s cancer centre be?” We are consulting on two options – that the future centre is either:
- at Evelina London Children’s Hospital, Lambeth, south London, with conventional radiotherapy services at University College Hospital, or
- at St George’s Hospital, Tooting, south London, with conventional radiotherapy services at University College Hospital.
We are consulting on this change because very specialist cancer treatment services for children – like those at The Royal Marsden’s site in Sutton – are now required to be on the same site as a children’s intensive care unit that can give life support. This is vitally important for lots of reasons which are explained in this document.
With the experience and expertise of specialist children’s cancer teams on the same site as children’s intensive care specialists, surgical teams and other children’s specialties, the future Principal Treatment Centre will minimise risk to children and be capable of giving innovative treatments that require intensive care support on site.
Our vision for the future centre is that it will:
- build on all the strengths of the existing service – high quality care by expert staff, good access to clinical trials, a family-friendly centre for children and young people, and ground-breaking research working very closely with the Institute of Cancer Research. These things are very important to children, families and staff.
- give best quality care and achieve world-class outcomes for children with cancer for decades to come.
There will be no sudden changes to how children and young people receive care. The future Principal Treatment Centre would not be ready until at least 2026. The move would be carefully planned with the full involvement of current teams and clear information for parents and families. We recognise, as with any move of service, there would be risks we need to manage, and planning for that is already underway.
Please share your views as part of this consultation. All the feedback we receive and other evidence will be fully considered by the NHS leaders who will take the decision on where the future centre will be.
Caroline Clarke
Regional Director, NHS England – London
Dr Chris Streather
Medical Director, NHS England – London
Jane Clegg
Chief Nurse, NHS England – London
Anne Eden
Regional Director, NHS England – South East
Dr Vaughan Lewis
Medical Director, NHS England – South East
Andrea Lewis
Chief Nurse, NHS England – South East

Who we are
This consultation is led by NHS England London and NHS England South East. We are two of NHS England’s seven regional teams. Between us, we are responsible for the quality of services and financial and overall performance of all NHS organisations in London and South East region.
We lead on planning and paying for specialised services, such as the services for children with cancer this consultation is about. We also oversee any substantial changes to health services in the capital and South East region. We make sure they offer clear health benefits and a good experience of care for patients, and are based on sound clinical evidence.

What is this consultation about?
Children’s cancer centres (known as Principal Treatment Centres) are responsible for making sure every child with cancer gets the expert care they need. They are mainly for children aged 15 and under with cancer (they can carry on caring for older children if that is best for individual patients.)
This consultation is about the centre for children with cancer living in Brighton and Hove, East Sussex, Kent, Medway, south London and most of Surrey. We describe this as “south London and much of the south east.” It is what we mean when we say “the catchment area.”
When we talk about cancer surgery in this document, we are not referring to bone, eye or liver cancer surgery or cancer-related neurosurgery which will continue to be provided at specific hospitals as happens now.
This document explains:
- why we need to change the location of specialist children’s cancer services
- our proposals for the future
- what children, parents, NHS staff and researchers have told us
- the options and what they each offer
- our preferred option
- how you can share your views and what happens next.
Please note we use alphabetical order to present both the list of places in the catchment area of the children’s cancer centre and information about the options. However, we do not refer to the current service in alphabetical order.
Current service
The Principal Treatment Centre for south London and much of the south east is currently provided in partnership between The Royal Marsden NHS Foundation Trust and St George’s University Hospitals NHS Foundation Trust. (Trusts are NHS organisations that run services for patients.)
The teams leading and coordinating specialist care for children with cancer, including chemotherapy, conventional radiotherapy and bone marrow transplants, are based at The Royal Marsden’s site in Sutton. Life-saving intensive care, high dependency beds (for children who need more support than is provided on a children’s ward), most children’s cancer surgery, and many other specialist services needed by children with cancer are led and coordinated by the teams at St George’s Hospital eight miles away in Tooting.
The service they provide is safe and high quality. The teams on the two sites work very hard to make sure children with cancer get safe, joined-up care. A children’s cancer consultant and a doctor from The Royal Marsden are at St George’s every day. The Royal Marsden’s children’s cancer consultants provide 24/7 cover for both sites and will attend at any time, if needed in an emergency.
St George’s surgeons carry out some surgical procedures at The Royal Marsden, and complex surgery and surgery on children at higher risk of complications at St George’s Hospital. A consultant endocrinologist (a doctor who specialises in hormones) from St George’s runs a clinic twice a week at The Royal Marsden.
Evelina London Children’s Hospital staff also run a weekly clinic at The Royal Marsden for children who need heart checks.
Children’s neurosurgery for cancers of the brain, nervous system and spine, and for complications of cancer treatment, is provided by King’s College Hospital and St George’s Hospital. They work closely together and with The Royal Marsden to care for these patients. Children travel for proton beam therapy (a very targeted form of radiotherapy) to University College Hospital, and for specialist surgery for specific cancers to a number of hospitals in London which are centres of excellence (see the future children’s cancer services section below for more details).
The Royal Marsden hosts the children’s cancer network, which coordinates and develops care provided in children’s cancer shared care units at more local hospitals across the Principal Treatment Centre’s catchment area (see the specialist centres table below for more information). These provide supportive care and, where agreed, specific chemotherapy treatments, as close to home as possible.
The Institute of Cancer Research, one of the world’s most influential cancer research organisations, is based next to The Royal Marsden’s sites in Chelsea and Sutton. Its teams undertake laboratory-based research to develop new drugs. They work closely with The Royal Marsden, which is a leading centre for cancer research, and St George’s Hospital. This helps turn discoveries made by scientists into new treatments for patients.
The Royal Marsden has a drug development unit for children and young people with researchers who oversee clinical trials – a way for children to get treatments that might not otherwise be available. Thanks to the role of many of The Royal Marsden’s consultants in national and international cancer networks, many children get access to new or innovative treatments as part of a clinical trial.

The proposed changes we’re consulting on
It is now a requirement for very specialist cancer treatment services for children to be on the same site as a children’s intensive care unit and other specialist children’s services.
As described above, the current service for children with cancer who live in south London and much of the south east does not and cannot meet this requirement. As a specialist cancer hospital, The Royal Marsden does not have a level 3 children’s intensive care unit (which can give life support) on site.
Children’s intensive care units are always on sites used by tens of thousands of children every year because intensive care teams need to see high volumes of very sick children to maintain their specialist skills and expertise. This wouldn’t be supported by the number of children treated at The Royal Marsden.
As the children’s cancer services currently at The Royal Marsden need to move, we are consulting on two options for the proposed future children’s cancer centre – Evelina London Children’s Hospital and St George’s Hospital. Depending on the decision, some specialist children’s cancer services currently provided by St George’s Hospital might move too.
We propose that, under both options, all radiotherapy services for the future children’s cancer centre (instead of some, as now) would be provided at University College London Hospitals NHS Foundation Trust (UCLH) in central London.
This consultation is about these proposed changes. We want to gather views, feedback and evidence to help with decision-making.
Why things have to change
Five main reasons
There are five main reasons why the specialist children’s cancer services at The Royal Marsden need to move be on the same site as a children’s intensive care unit.
The current Principal Treatment Centre does not meet national requirements
National clinical requirements for Principal Treatment Centres are set by NHS England. They say very specialist cancer treatment services for children – like those at The Royal Marsden – MUST be on the same site as a level 3 children’s intensive care unit and other specialist children’s services. This is non-negotiable. The current Principal Treatment Centre does not and cannot comply.
The national service specification for Principal Treatment Centres was approved by NHS England in 2021 after being developed with patients, parents and professionals.
Hospital transfers of very sick children for intensive care add risks and stress
Every year, a small number of very sick children who need intensive care are transferred eight miles from the specialist children’s unit at The Royal Marsden’s Sutton site to St George’s children’s intensive care unit at Tooting.
This is done safely. But urgent transfers of very sick children to another hospital for level 3 intensive care services that can give life support, even in a special children’s ambulance with an expert team on board, add risks to what is already a very difficult situation. These risks can only ever be managed. Transfers of very sick children also put added stress on patients, parents, and the staff involved.
Patient transfers from shared care units in local hospitals to the specialist children’s cancer centre, including emergency patient transfers, would not be affected by our proposals. By their nature, most shared care units are a long way from the specialist centre. They are all on sites which have beds where children can be closely monitored and given support. Children are only transferred for level 3 care when it is unavoidable.
The intensive care team is not currently able to provide face-to-face advice on the care of children on the ward
Currently, the Principal Treatment Centre’s intensive care specialists are at St George’s Hospital while most specialist care for children with cancer is at The Royal Marsden. Some children every year have to be transferred by ambulance from The Royal Marsden to the cancer ward at St George’s Hospital as a precaution, in case they suddenly get worse and need intensive care. It can be disruptive and stressful for them.
Intensive care specialists can’t work closely with specialist cancer teams to help children stay well enough to avoid intensive care if they are not all on the same site.
There is a need to improve children and families’ experience when patients require intensive care and other specialist children’s services
Some specialist children’s services needed by children with cancer are not on site at The Royal Marsden, because it is a specialist cancer hospital. Staff at The Royal Marsden arrange for children to attend or be safely transferred to other hospitals as needed.
Parents and staff say having to get to know new members of staff at different locations, especially at a time of crisis, can increase families’ anxiety and distress.
Children’s cancer care is complex. Our proposals would not eliminate the need for children to get specific kinds of expert care at different hospitals (see more information in the future children’s cancer services section below). Under our proposals, conventional radiotherapy would move to University College Hospital. Instead of some (as now), all children who need radiotherapy would go to University College Hospital.
Although it offers a wide range of innovative treatments, the current Principal Treatment Centre is excluded from giving a specific type of new treatment, and others expected in the future
Innovative cancer treatments are bringing new hope for children and families. Some have a greater risk of complications – such as too big a response from a child’s immune system – that could require urgent support from an on-site intensive care team. As a result, they can only be given at children’s cancer centres on the same site as a children’s intensive care unit.
This is the case for ground-breaking CAR-T treatment, which uses a child’s own, treated, cells to fight their cancer. Many more of these treatments are expected to become available in the next few years.
The Principal Treatment Centre for south London and much of the south east is currently excluded from giving these life-saving treatments. There is a compelling case to move the centre so it has the same opportunity to provide future treatments as other major centres worldwide.

Who would this affect?
About 1,400 children, most aged one to 15, are under the care of the Principal Treatment Centre at any given time. More than 60% of the centre’s patients are from outside London. About 190 children aged one to 15 living in south London and much of the south east are diagnosed with cancer every year.
We used data from 2019/20 for an in-depth look at the service (a check in 2021/22 showed numbers were still very similar).
- 1,373 children were treated by the Principal Treatment Centre in 2019/20
- 536 had inpatient care (they were admitted to The Royal Marsden or St George’s for day care or a stay of at least one night)
- 1,367 had outpatient care (they came to The Royal Marsden or St George’s for an appointment)
- 84 had intensive care (15 came from The Royal Marsden, others were already at St George’s or were transferred there from their local shared care unit)
- 41 had conventional radiotherapy at The Royal Marsden.
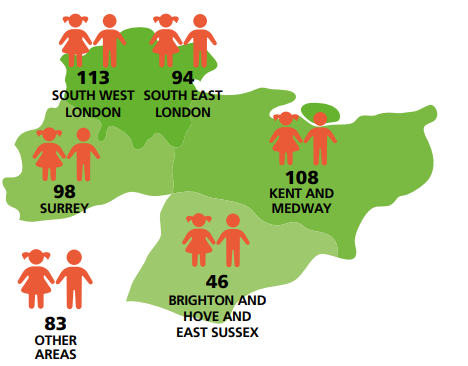
In 2019/20, the Principal Treatment Centre treated 536 children as inpatients (many had care at both hospitals):
- 113 children from south west London
- 108 children from Kent and Medway
- 98 children from Surrey
- 94 children from south east London
- 46 children from East Sussex and Brighton and Hove
- 83 children from other areas.
This map shows the catchment area for the centre and the number of inpatients from each area who used it in 2019/20.
The number of children attending for outpatient care followed a similar pattern.
About 15% of patients are children who live outside the catchment area but choose to be treated by the centre. This includes some patients from West Sussex whose nearest shared care unit is at Redhill, Surrey, which comes under the current Principal Treatment Centre at The Royal Marsden and St George’s.
An overview of the Principal Treatment Centre
This table shows how many children used the different services at The Royal Marsden and St George’s Hospital in 2019/20 (many children went to both hospitals)
| Type of care | St George’s Hospital | St George’s Hospital | The Royal Marsden | The Royal Marsden | Total | Total |
|---|---|---|---|---|---|---|
| Number of patients | Number of visits/days in hospital | Number of patients | Number of visits/days in hospital | Number of patients | Number of visits/days in hospital | |
| Inpatient including day cases including: | 208 | 313 visits | 456 | 4,599 visits | 536 | 4,912 visits |
| Planned care with at least one night in hospital | 72 | 90 visits | 147 | 412 visits | 191 | 502 visits |
| Unplanned care with at least one night in hospital | 93 | 115 visits | 44 | 50 visits | 136 | 165 visits |
| Outpatient | 72 | 275 visits | 1,354 | 7,943 visits | 1,367 | 8,218 visits |
| Intensive care | 84 | 1,451 bed days | 84 | 1,451 bed days | ||
| Conventional radiotherapy | 41 | 700 visits | 41 | 700 visits | ||
| Total | 210 | 1,356 | 1,373 |
This table shows how often children from the different areas went to The Royal Marsden or St George’s Hospital for any kind of care in 2019/20. More than one in ten children had over 20 visits and a few had over 50.
| Number of visits by patients from each area | 1 | 2 | 3 | 4 | 5 | 6-10 | 11-15 | 16-20 | 21-30 | 31-40 | 41-50 | 51+ |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Brighton and Hove | 5 | 2 | 3 | 4 | 2 | 10 | 4 | 3 | 1 | |||
| East Sussex | 9 | 9 | 9 | 5 | 4 | 11 | 12 | 3 | 2 | 5 | 5 | |
| Kent and Medway | 61 | 51 | 39 | 21 | 8 | 53 | 24 | 9 | 13 | 10 | 4 | 9 |
| South east London | 52 | 38 | 27 | 17 | 15 | 36 | 27 | 12 | 12 | 5 | 5 | 6 |
| South west London | 39 | 39 | 27 | 21 | 11 | 38 | 26 | 13 | 16 | 13 | 7 | 8 |
| Surrey Heartlands (excludes Farnham, Surrey Heath) | 43 | 39 | 30 | 12 | 10 | 36 | 15 | 18 | 15 | 5 | 4 | 5 |
| West Sussex | 14 | 16 | 12 | 12 | 7 | 13 | 4 | 1 | 4 | 3 | 4 | 2 |
| Other | 27 | 29 | 13 | 22 | 11 | 67 | 33 | 31 | 23 | 9 | 14 | 21 |
| Percentage of visits % | 18 | 16 | 11 | 8 | 5 | 16 | 9 | 5 | 5 | 3 | 2 | 3 |
Background information
Anonymised data from individual children who used the Principal Treatment Centre in 2019/20 was used to understand patients’ journeys and experience for this consultation.
Overall, we don’t expect any growth in the number of children needing cancer services over the next 20 years. Though the proportion of children diagnosed with cancer is expected to go up slightly, the overall number of children aged 15 and under in the catchment area is expected to fall. So the need for children’s cancer services will stay steady.
Our proposals
Overview
Under our proposals, the children’s cancer services and clinical trials that are based at The Royal Marsden would transfer to a hospital which already has children’s intensive care and other specialist children’s services. Under both options, all radiotherapy services for the future children’s cancer centre (instead of some, as now) would be provided by University College London Hospitals NHS Foundation Trust. This would happen within two and a half years of the decision if all goes smoothly. We expect all the preparations for the future Principal Treatment Centre to be undertaken during that time, including building work, equipping the centre and putting everything in place for a safe, smooth transfer.
Our process to identify possible ways of providing very specialist cancer treatment services for children which are currently at The Royal Marsden is described in the developing and assessing our shortlist of options section below. It found one solution that met all the criteria. This is that the future service must be based at an existing hospital in south London that provides specialist children’s services and has a children’s intensive care unit. This has led to the two options in this consultation. They are for the future Principal Treatment Centre to be at either:
- Evelina London Children’s Hospital which is part of Guy’s and St Thomas’ NHS Foundation Trust, or
- St George’s Hospital which is part of St George’s University Hospitals NHS Foundation Trust as well as St George’s, Epsom and St Helier Hospitals and Health Group.
Research for new drugs and treatments would continue at the Institute of Cancer Research in Sutton, working closely with staff at the future Principal Treatment Centre.
When this document talks about ‘the two Trusts’ or ‘both Trusts’, we are referring to Guy’s and St Thomas’ NHS Foundation Trust, and St George’s University Hospitals NHS Foundation Trust. What children, parents and staff told us helped to shape our proposals for the future Principal Treatment Centre. To find out more about what they said and what we did, see the what children, parents and staff have told us section below.
Wherever it is, the future children’s cancer centre will:
- meet the national clinical service specification, with all the benefits that brings
- provide excellent patient and parent/carer experience, including being child-friendly and having good facilities for parents and families
- have lots of experience and expertise at supporting patients and families to deal with complex services, including at other hospitals, and through times of extreme difficulty
- look after and develop its staff who are vital to the service, providing good training and opportunities, and additional support such as a nursery for childcare
- have the staff, expertise, space and equipment to give children and young people all the care that they need, 24 hours a day, 365 days a year, and have plenty of experience of listening to children, young people and families to make services better
- aim to further increase participation in cutting-edge clinical trials
- make sure there are really good, flexible, personal arrangements for children moving into teenage and young adult services and that no one falls through the gaps
- continue the current focus on increasing rates of ‘banking’ (storing) more tissue from children’s tumours, enabling more research into possible new treatments
- continue the current focus on making greater use of genomic medicine allowing treatments to be tailored to children’s own individual DNA and diagnosis
- lead and support close, joined-up working between different children’s cancer services so children get access to care when and where they need it, wherever they live. This would include supporting the shared care units within the children’s cancer network for south London and much of the south east.
We believe we can achieve all this through the hard work and focused efforts of all our organisations and crucial partners like the Institute of Cancer Research.

Future children’s cancer services – what would be where
If Evelina London became the future Principal Treatment Centre, it would have all the specialist children’s cancer services currently at The Royal Marsden (except conventional radiotherapy) and the specialist children’s cancer services currently provided for the Principal Treatment Centre at St George’s alongside its well-established children’s intensive care unit and other specialist children’s services.
If St George’s became the future Principal Treatment Centre, it would have all the specialist children’s cancer services currently at The Royal Marsden (except conventional radiotherapy) alongside its well-established children’s intensive care unit and other specialist children’s services, including the services it already provides for the Principal Treatment Centre.
Under both options, St George’s would continue to provide a children’s cancer shared unit for local children, and its neurosurgery services. We propose that, under both options, all radiotherapy services would be provided by University College Hospital. Children would continue to travel for some specialist cancer services because of the specific expertise hospitals have in these areas.
The table below shows what would be where.
| Children’s cancer services which the national service specification says must be on site at a Principal Treatment Centre | On site for current service at The Royal Marsden | Would be on site for proposed future Principal Treatment Centre if it was at Evelina London Children’s Hospital | Would be on site for proposed future Principal Treatment Centre if it was at St George’s Hospital |
|---|---|---|---|
| Children’s anaesthetics and pain management | Yes | Yes | Yes |
| Children’s blood cancer (haematology) services | Yes | Yes | Yes |
| Children’s cancer (paediatric oncology) services including diagnosis, chemotherapy, bone marrow transplants, ongoing monitoring and care | Yes | Yes | Yes |
| Children’s cancer pharmacy services | Yes | Yes | Yes |
| Children’s radiology services (such as CT and MRI scans) | Yes | Yes | Yes |
| Children’s surgery, including management of emergencies, central lines and biopsy services | Partially – most surgery is at St George’s | Yes | Yes |
| Level 3 critical care (can provide life support) | No – patients go to St George’s | Yes | Yes |
| Therapy services such as psychology and physiotherapy | Yes | Yes | Yes |
| Services which the national service specification says do not need to be on-site but must be readily available at all times | On site for current service at The Royal Marsden | Would be on site for proposed future Principal Treatment Centre if it was at Evelina London Children’s Hospital | Would be on site for proposed future Principal Treatment Centre if it was at St George’s Hospital |
|---|---|---|---|
| Inpatient cardiology (for patients with defects and diseases of the heart and blood vessels) | No – patients go to Evelina London | Yes | No – patients would go to Evelina London for specialist care |
| Children’s cancer surgery (to remove or reduce tumours and manage some cancer-related symptoms) | No – patients go to St George’s | Yes | Yes |
| Children’s infectious disease services | No – patients go to St George’s | Yes | Yes |
| Children’s pathology (investigates and identifies cancers) | Yes | Yes | Yes |
| Endocrinology (for patients with hormone-related disease) | Yes | Yes | Yes |
| Gastroenterology (for patients with diseases of the digestive system) | No – patients go to St George’s | Yes | Yes |
| Genomic testing* (finds changes in genes causing cancer) | Yes | Yes | Yes |
| Inpatient nephrology (for patients with kidney disorders) | No – patients go to Evelina London for specialist care | Yes | No – patients would go to Evelina London for specialist care |
| Neurosurgery (for cancer-related problems affecting patients’ brains, nervous systems or spines) | No – patients go to King’s or St George’s | No – as now, patients would go to King’s or St George’s | Yes – as now, patients would go to King’s or St George’s |
| Ophthalmology (for patients with eye and visual disorders) | No – patients go to St George’s | Yes | Yes |
| Other specialist children’s surgery (apart from the types of surgery listed below) | No – patients go to St George’s | Yes | Yes |
| Palliative care (aims to give a good quality of life for patients living with an illness that cannot be cured) | Yes | Yes | Yes |
| Radiotherapy (uses radiation to kill cancer cells) | Partially – patients have conventional radiotherapy on site but go to University College London Hospitals for proton beam and other types of specialist radiotherapy | No – patients would go to University College Hospital for all radiotherapy | No – patients would go to University College Hospital for all radiotherapy |
* The Clinical Advisory Panel of experienced clinicians who helped us develop the options defined services that must be ‘readily available’ for a Principal Treatment Centre (the wording in the service specification) as ‘available on site within 30 minutes’. The panel decided this did not apply to genomic testing so genomic testing was not assessed for our pre-consultation evaluation.
| Cancer services for children and young people which are not part of this consultation | Specialist centres |
|---|---|
| Bone cancer surgery | Royal National Orthopaedic Hospital, Stanmore, north London |
| Care for babies aged 0 to 12 months with cancer of any type | Great Ormond Street Hospital for Children, Bloomsbury, central London |
| Eye cancer surgery | Royal London Hospital, Whitechapel, east London |
| Liver cancer surgery | King’s College Hospital, Camberwell, south London |
| Neurosurgery: surgery on the brain, nervous system and spine. It is usually for children with cancers of the brain, nervous system or spine but can sometimes be for complications in children with other kinds of cancer | Neurosurgery is provided by King’s College Hospital, Camberwell, south London and St George’s Hospital, Tooting, south London. The neurosurgery service each of them provides is a key part of services for children in south London and much of the south east, including as part of the trauma services at both hospitals for children who have been badly injured. They both work closely together and will continue to do so. In 2019/20, 86 children had cancer-related neurosurgery. Around 20% of children had their neurosurgery at St George’s. Although numbers do vary year on year, the proportion of neurosurgery that both sites do is expected to remain similar. |
| Proton beam radiotherapy and other superspecialist radiotherapy services | University College Hospital, near Euston, central London |
| Hospitals where these services are provided | |
| Children’s cancer shared care units in Kent, Medway, south London, Surrey and Sussex which provide supportive care and, where agreed, specific chemotherapy treatments, liaising closely with the specialist children’s cancer centre | Conquest Hospital, Hastings, East Sussex Croydon University Hospital, Croydon, south London East Surrey Hospital, Redhill, Surrey Epsom Hospital, Epsom, Surrey King’s College Hospital, Camberwell, south London Kingston Hospital, Richmond, south London Medway Maritime Hospital, Gillingham, Medway Queen Elizabeth Hospital, Woolwich, south London Queen Elizabeth the Queen Mother Hospital, Margate, Kent Royal Alexandra Children’s Hospital, Brighton Royal Surrey County Hospital, Guildford, Surrey St George’s Hospital, Tooting, south London St Peter’s Hospital, Chertsey, Surrey Tunbridge Wells Hospital, Pembury, Kent William Harvey Hospital, Ashford, Kent |
| Teenage and young adult services for 16 to 24 year olds | The Royal Marsden Hospital in Chelsea and Sutton |
Proposed changes to radiotherapy services
Radiotherapy is a treatment where external beam radiation is used to kill cancer cells. Many children diagnosed with cancer need this as part of their treatment.
There are different types of radiotherapy treatment. Most children who need radiotherapy currently have conventional radiotherapy (mostly using high-energy x-rays also known as ‘photon beams’). This is delivered for children under the care of the current Principal Treatment Centre by the specialist team at The Royal Marsden. University College London Hospitals NHS Foundation Trust’s specialist teams provide the other types of radiotherapy for these children, including ‘proton beam’. The only other place in England which provides proton beam therapy is in Manchester.
Though it is only suitable for certain types of cancer, proton beam therapy precisely targets tumours, reducing damage to healthy tissue and potentially reducing long-term side-effects. As the very specialist proton beam therapy service develops, more children with cancer are expected to benefit from it, with fewer children having conventional radiotherapy.
While The Royal Marsden service currently provides high quality conventional radiotherapy treatment for children as part of their care, the proposed move of specialist children’s cancer services to either Evelina London or St George’s, alongside advances in radiotherapy treatment, means we propose this service is provided differently in the future.
This is because:
- it would be difficult to sustain the conventional radiotherapy service for children at The Royal Marsden without the staff and facilities of the Principal Treatment Centre on site
- we also expect the number of children requiring conventional radiotherapy services in the future to fall, meaning a high quality service would be even harder to sustain.
We therefore need to consider proposals for the future provision of conventional radiotherapy services as part of this consultation.
In both options, we therefore propose that (as part of the overarching changes for specialist children’s cancer services) conventional radiotherapy moves from The Royal Marsden to University College Hospital, located on Euston Road in central London. All radiotherapy (conventional as well as proton beam and other types) rather than some, as now, would then be provided as part of a larger combined service at University College Hospital. Our proposals do not affect radiotherapy services for 16 to 24 year olds, or adult services provided at The Royal Marsden.
Radiotherapy already works like this for children who go to the Principal Treatment Centres at Great Ormond Street Hospital and Southampton, and some patients from Oxford. The details of how this would work in practice to give patients the best care and experience would be agreed by clinicians and managers. NHS England would support the development of these plans.
Bringing all radiotherapy services together on the same site at University College Hospital would create opportunities to improve care for children with cancer (see the radiotherapy benefits section for more information). It would also have some other impacts. These would include some transfers that don’t happen now and longer journeys for some children and their families compared to now (more information on this can be found in our travel section below).
- Up to 10 children a year who have radiotherapy ahead of a bone marrow transplant (total body irradiation which often needs to be provided during a hospital stay) would have a planned transfer from the future centre to University College Hospital for this treatment.
- Around 25 other children with cancer every year would go to University College Hospital for conventional radiotherapy as outpatients or day cases, travelling from home and back, instead of going to The Royal Marsden (as now). Numbers would vary year on year.
More information about radiotherapy is available on our radiotherapy services page.
What would the proposed changes mean?
Benefits
Whether the future Principal Treatment Centre was at Evelina London or St George’s, it would:
- end hospital transfers from the specialist centre of very sick children who need or might need intensive care, eliminating the added risks and stress these transfers bring. If children did need an intensive care bed, the intensive care unit would be very close by on the same site
- enable children to get more of their care on the specialist cancer ward and minimise the number of children admitted to intensive care, which can be stressful for children and families. With intensive care specialists on site:
- children would never be transferred as a precaution in case they might go on to need intensive care.
- specialist input from intensive care teams could help some children avoid intensive care. Cancer specialists say cancer services in children’s hospitals with intensive care units on site have fewer intensive care admissions for this reason.
- have more services on the same site than now, improving experience for many children and families
- meet the national requirements and be capable of offering cutting-edge treatments that need intensive care on site
- make it easier for different specialist teams treating the same child to work closely together, improving care for children and supporting new kinds of research too
- make it easier for cancer and non-cancer specialists to learn from each other and share learning. As well as being good for children’s care, this would be likely to help the future centre keep and attract new staff.
Between 1 April 2019 and 31 March 2020
- 456 children with cancer were treated as inpatients at The Royal Marsden
- 35 children were taken by ambulance from The Royal Marsden to St George’s Hospital because they needed or might need intensive care
- 15 children were treated in the intensive care unit
- 23* children were treated on the ward
- 50 ambulance journeys took these children between the two hospitals
*During the year, a few children were transferred more than once from The Royal Marsden to St George’s because they needed or might need intensive care. Some of them had different types of care on different occasions. This is why the numbers of children having different types of care are more than the total number of children who were transferred.
After these changes
0 children would need to be taken from the specialist centre to another hospital for intensive care.

Radiotherapy benefits
Under both proposals, conventional radiotherapy for children with cancer would move from The Royal Marsden to University College Hospital, bringing together all radiotherapy services on one site, instead of two as now. This would mean:
- more opportunities for doctors and other professionals to work together in one place, allowing them to develop greater expertise and specialist knowledge in treating cancer and improve outcomes for patients.
- as a bigger combined service, joining up in this way would also help ensure the service could be provided to children when they needed it, even when some staff had time away from work
- more opportunities to undertake different kinds of research (clinical and lab-based) to improve future care for children.
Things we would need to focus on
Whether the future Principal Treatment Centre was at Evelina London or St George’s, there would be some challenges as there are with moving any service. They would need to be well managed. All organisations involved are committed to working closely together.
We all share the same objective, to ensure the very best service is provided for children and families, and that the change that needs to be made does not interrupt care. This will be an important part of our ongoing work. Early planning for how the proposed changes would be made has already started. There will be much more detailed planning once a decision on the location of the proposed future centre has been made. It will be the key focus during the two and a half years until the service transfers, and afterwards too.
Some of the things that we will focus on managing are:
- keeping the current high level of research and funding for research going at the future centre; for instance, without careful management it could be difficult to maintain the same level of grant funding, staffing and the benefits of the children’s cancer centre being located next door to the Institute of Cancer Research (as it is at The Royal Marsden) at least at first
- supporting as many as possible of the experienced and expert staff who provide the service to move to the future centre, and to feel part of their new organisation. With the current proposals, this would certainly affect staff who provide children’s cancer care at The Royal Marsden. Depending on the decision, staff at St George’s Hospital could be impacted too. Where staff did not transfer, plans would also need to be put in place to fill gaps and ensure that the expertise of these staff is not lost to the NHS.
- ensuring The Royal Marsden has strong plans for continuing teenage and young adult services and that the move to its teenage and young adult services (usually around the time of a child’s 16th birthday) continues to go smoothly.
However important it is to move a service, it may be disruptive and upsetting for the people involved. Everyone cares very deeply about children’s cancer care.

Travel is also something parents and staff have raised concerns about. More information is available on this on our ‘How travel times were assessed and scored for this consultation’ page. Being aware of these things means that we can work together to manage them.
For instance, some research and other staff at The Royal Marsden are funded by The Royal Marsden’s charity. Both Evelina London and St George’s have considered this in their plans. They both have hospital charities which would work closely with the future Principal Treatment Centre if it is on their site.
The Royal Marsden and St George’s teams, alongside the future Principal Treatment Centre (wherever it is located) would make sure staff and families have the support they need through this time of change and that the service runs smoothly throughout, including for children moving on to teenage and young adult services. They would work with families on preserving memorials for children in line with families’ wishes.
The future centre (wherever it was located) would work closely with the Institute of Cancer Research and research staff at The Royal Marsden and St George’s to develop ways of working that support research to continue and thrive. These would include close engagement with organisations which fund research and trials to build confidence in future arrangements, and planning to make the best use of the expertise that staff have and to build new relationships, data and sample handling arrangements.

Impacts of these proposed changes on different groups
As the Principal Treatment Centre covers a wide area, the move of The Royal Marsden’s services would improve access for some families and make it harder for others.
We carried out an initial equality and health inequalities impact assessment (EHIA) to help us understand how what we do may affect different groups of people in different ways.
This found the benefits of having specialist children’s cancer services on the same site as intensive care, cancer surgery and other specialist children’s services may be even greater for:
- children with a higher need for treatment by other children’s specialties (such as those with complex cancer care needs, who are disabled or have other health conditions)
- families with language barriers or poor literacy who find attending several sites particularly difficult.
It also highlighted potential negatives:
- the cost, complexity and length of journeys and parking issues for many families (for both potential sites for the future centre and University College Hospital for radiotherapy services)
- patient and carer worries about the change and getting used to a new site.

Families who are struggling financially, who do not speak English or who have disabilities are more likely to find the change difficult. Hastings in East Sussex, much of south east London, and Swale and Thanet in Kent have the largest numbers of families living in difficult circumstances although every part of the catchment area has some.
The impact assessment made recommendations for things that could make the change easier for children and families. These include:
- help for patients and families to plan their journeys to hospital, including easy to understand information in different languages
- getting their travel costs paid quickly. Help to access other financial support
- improving non-emergency transport services for patients and their families
- space for families to stay
- easy arrangements at the site, including for dedicated parking and drop-off
- convenient appointment times, more care closer to home, strong communication between different health and social care teams, and online or phone appointments
- an excellent plan to support patients during the move, with a named care coordinator (such as a specialist cancer nurse) for each child and family.
The team running the future centre will need to act on these recommendations. Everyone involved is committed to doing so.
Our equality and health inequalities impact assessment will be further updated after the consultation to help with planning the future Principal Treatment Centre, including the proposed move of radiotherapy services.
Stories of the present and future
These are examples – not the stories of actual patients.
Eva’s story
Background
Eva is an 11-year-old girl who lives with her parents in Hastings, East Sussex. She has acute myeloid leukaemia. Her specialist cancer care is led by the Royal Marsden NHS Foundation Trust.
Eva is having her first cycle of chemotherapy treatment at The Royal Marsden.
A few days ago, she caught a virus. Despite taking extra antiviral medication, Eva developed fevers and a dry cough.
Yesterday morning she was getting very tired from the increased effort she was making to breathe. The level of oxygen in her blood dropped and her heart rate increased. To help with her breathing, Eva needed oxygen via a face mask.
Now
The paediatric team at The Royal Marsden follows strict guidelines when children have breathing problems. If a child may need intensive care treatment, conversations with other professionals start at an early stage. Staff call the South Thames Retrieval Service (STRS) to transfer the child to St George’s Hospital in a specially equipped children’s ambulance.
Eva was transferred to St George’s children’s intensive care unit.
Every day, a children’s consultant from The Royal Marsden attends St George’s Hospital to look after children with cancer and share their expertise with the teams treating children with cancer.
Today, the haematology consultant (who treats blood cancers) is giving guidance to the intensive care team about some of the specialist medication Eva needs. This will reduce her chances of having other complications from her treatment.
The consultant is delighted to hear that Eva’s condition has improved. She is now stable without requiring oxygen. Her temperature has settled, and her heart is beating at a normal rate and rhythm for her age.
The children’s intensive care team suggests Eva may be able to return to The Royal Marsden in a day or two. Eva will go on to have three more cycles of chemotherapy at The Royal Marsden. After each of them, she will go home.
If, when all her chemotherapy treatment is finished, Eva needs a bone marrow transplant, she will have it at The Royal Marsden.
In the future
At the future Principal Treatment Centre, children’s cancer services currently at The Royal Marsden would be on the same site as children’s intensive care.
Staff from the children’s intensive care unit would be able to support the medical and nursing team looking after Eva on the cancer ward. This might mean she would not need to go to the children’s intensive care unit.
If her symptoms got worse and she did need intensive care, there would be no journey by ambulance to another hospital: she would simply be moved to the intensive care unit nearby. Cancer specialists would be able to visit Eva regularly to monitor her progress and advise the intensive care team throughout her time in intensive care.
Eva would go on to have the rest of her chemotherapy at the future Principal Treatment Centre. If, when all her chemotherapy treatment was finished, Eva needed a bone marrow transplant, she would have it at the same hospital.
Wherever she was in the hospital, the key members of staff involved in her treatment and the same team of play specialists and teachers would all continue to see Eva regularly.

Ravi’s story
Background
Ravi is an eight-year-old boy who has a tumour in one of his kidneys. He lives with his mother and little sister in Ramsgate, east Kent.
When Ravi was first diagnosed, he had an operation at St George’s Hospital in Tooting to insert a portacath (a device used to take blood and give treatments).
Then he had chemotherapy for four weeks at The Royal Marsden NHS Foundation Trust in Sutton.
He has recently had a second operation at St George’s where specialist children’s surgeons removed the cancer from his kidney.
He, his mum and sister travel to the hospitals by hospital transport. It takes at least an hour and a half to get to Sutton and around two hours to reach Tooting.
Now
Ravi needs a further 12 courses of chemotherapy. This will mean three days of chemotherapy treatment at The Royal Marsden, every three weeks, for 34 weeks. There are flats for patients and families nearby where he and his family can stay if needed.
Chemotherapy can affect fertility. Ravi’s consultant has suggested he has an operation at St George’s in case he wants to have children in the future. This will be before he starts chemotherapy.
Because Ravi is so young there may be long term effects of treatment. So he will also need regular hearing assessments, kidney function tests, and echocardiograms (a scan to look at the heart and surrounding blood vessels) to check for any changes.
The kidney tests and echocardiograms will be at The Royal Marsden. The hearing assessments will be at a special centre.
This will mean Ravi and his family travelling to up to two different hospitals and the hearing centre before he starts chemotherapy and at specific points during his treatment.
A clinical nurse specialist at The Royal Marsden will make the appointments, help with the arrangements and offer expert support and care to Ravi and his family. But travelling to different sites can be a stressful experience for families.
In the future
At the future Principal Treatment Centre, very specialist cancer treatment services for children would be on the same site as children’s cancer surgery and most other specialist services that children with cancer need.
Ravi’s surgeries and treatments would be in one place that he already knows, which would improve the experience of care for Ravi and his family.
He would go to a different site if he needed radiotherapy. One in three children with his condition do.
It would take Ravi and his family about two hours to get to either of the two possible options for the future centre by road. Both options would also provide family accommodation, if needed.

What children, parents and staff have told us
We are working with patients, parents, health professionals, lead researchers and others to ensure the very best service for children’s cancer care into the future. Their knowledge and experience over the past three years have been invaluable. The conversations will continue after this consultation. We are very grateful for all their insights and guidance.
What do patients and families say?
Children with cancer and their parents and carers want specialist cancer services to provide:
- access to the best treatments and to specialists who are highly knowledgeable about their specific cancers
- child-friendly communications, care and environment with good facilities for children of different ages, and for parents
- access to clinical trials and the latest interventions
- to see staff they know
- quick, simple, stress-free travel to hospitals
- access to other services including mental health support.
Children particularly flag the importance of:
- feeling cared for during visits
- the quality of the food
- the impact of treatment on their stress and mental health.
Parents and carers highlight:
- the quality of cancer care their children receive
- worries about how immunosuppressed children will be kept safe
- worries about travel to the future centre.
“You said, we did”
A survey undertaken on our behalf with children, young people and parents in south London and much of the south east, and other engagement, including with our Stakeholder Group, helped us to identify the aspects of patient and carer experience the options appraisal looked at.
We also analysed travel times for families. You can find out more in our travel section below.
What do staff and researchers say?
We are speaking to staff at Evelina London, St George’s and The Royal Marsden to understand their views and concerns.
Staff who are part of the current Principal Treatment Centre say they want the future centre
- to keep giving patients excellent care
- to keep doing really strong research
- to provide staff benefits (such as childcare and opportunities for staff learning and development) at least as good as the ones they currently get.
They are concerned about:
- staff leaving the service
- travel times and costs of getting to the future Principal Treatment Centre
- the impact on wider services (such as radiotherapy and Teenage and Young Adult services).
They have some questions about how services would be delivered in the future (this will be looked at in great detail as part of planning the move).
Staff who spend more than half their time on children’s cancer care have the right to transfer to the future centre if they want to.
- 248 staff across The Royal Marsden and St George’s Hospital work in the service
- about 170 Royal Marsden staff would qualify to transfer to the future centre, if they wanted to
- if the future centre was at Evelina London rather than St George’s, four staff from St George’s would also qualify to transfer to the future centre, if they wanted to.
Evelina London staff do not currently provide specialist children’s cancer services so would not move under either option.
We hope that most staff who currently work in the Principal Treatment Centre would want to continue to provide care to children with cancer by moving to the future centre. Supporting them to do so is really important. We are meeting with staff to hear their concerns and answer their questions. We will continue to do this during and after the consultation.
Both Evelina London and St George’s are highly respected hospitals with strong track records of looking after their staff. Both would provide many opportunities for children’s cancer staff. These would include the chance to work with and learn from colleagues with different expertise, supporting their development.
However, experience of previous service changes shows that not all staff would want to move. We have to be realistic about this. During the two and a half years before the service transferred, plans would be drawn up to fill gaps. As Evelina London is not currently involved in providing many of the services for the current centre, it could have more planning work to do.
You said, we are doing – consultation plan
Staff wanted to know how staff benefits in the future might compare with now, so we asked the two Trusts about this. We also analysed travel times for staff. You can find out more in our travel section below.
What do research staff say?
Access to cutting-edge research is a key priority for the future Principal Treatment Centre. So two independent clinical experts spoke to senior researchers from The Royal Marsden, the Institute of Cancer Research, Trusts and associated universities. They asked for their views on how the research offer of the two options for the future centre should be evaluated. This feedback shaped the questions we asked the two Trusts.
We are also speaking to research teams at The Royal Marsden and the Institute of Cancer Research, to understand their views and concerns.
Staff who are part of research teams including at the Institute of Cancer Research say they want the future centre
- to keep giving patients excellent care
- to keep doing really strong research
They are concerned about:
- the need to find new ways of working across different sites and with new partners that are as good as now, so that research is not impacted
- possible disruption to clinical trials before and after the move to the future Principal Treatment Centre.

What we are doing
We are taking all these concerns very seriously. In planning this consultation, we have already taken a lot of actions to address the feedback we have had. You can read more about this in our pre-consultation feedback report. The consultation will also be an opportunity for people to highlight areas in our proposals that they are anxious or worried about. We will use this information to help develop our plans to make sure we address people’s concerns and give families, children, staff and researchers the support they need.
Hearing other views
It is important that any proposed service change like this is reviewed by clinical and other experts before we consult on our proposals. We also need to make sure the proposals satisfy the government’s and NHS tests. In this case, the London Mayor’s tests also apply, although only to any impacts on Londoners.
Our clinical and project teams have worked with the London and South East Clinical Senates. They are expert groups of senior clinicians who know the London and South East regions well and can offer an independent view. They have tested our proposals and given us helpful advice. You can read more about this in their report.
We are working with experts in NHS England, and the London Mayor to make sure our proposals are robust and satisfy all these tests.
We are also working with overview and scrutiny committees across the catchment area. These are run by local authorities and have a formal role in reviewing NHS plans. Brighton and Hove, East Sussex, Kent, Medway, and West Sussex Health Overview and Scrutiny Committees have asked to be involved but do not see this as a significant change for their residents. The South East London, and South West London and Surrey Joint Overview and Scrutiny Committees see it as a significant change for their residents and will be responding formally to our consultation.
Public consultation
Children, parents, staff, overview and scrutiny committees, children’s cancer charities and others have also given us advice on our consultation plan.
You said, we are doing – consultation plan
As the result of feedback, for the consultation we are:
- increasing our focus on speaking with and hearing from groups who can find it hard to access health services, and from new mothers/families with young children
- asking families in waiting rooms at Evelina London, St George’s and The Royal Marsden for their views
- offering visits to both Evelina London and St George’s for children, parents and staff
- sharing posters with QR codes to provide easy links to our documents and information about these proposals
- making sure people can find out about our consultation in lots of different ways.
Developing and assessing our shortlist of options
Over the past three years, we have had more than 730 responses about our proposals, via meetings, conversations, emails, surveys and workshops. They include responses from children, families and staff with a range of ages, ethnic backgrounds, languages, and experience of the current Principal Treatment Centre. We have been advised by four advisory groups including one of parents, charities and nurses, and one of clinicians; and a further independent Clinical Review Group of cancer specialists.
The work is overseen by the Programme Board (which is made up of leaders from the hospitals involved, senior doctors from within NHS England London and South East regions and external experts).
From long list to shortlist
With the support of different working groups and people, we have followed a best practice approach to understand the possible solutions for the future centre, by:
- agreeing a list of things that would not be affected by the service change (such as specific kinds of expert care at different hospitals), which we have called ‘fixed points’
- agreeing basic things that need to be delivered by any option we put forward, which we have called ‘hurdle criteria’. They include:
- the need for the service to be based in Greater London so it is accessible for everyone across the catchment area
- the ability to deliver the future centre within two and a half years of final go-ahead
- the need for the option to be affordable.
- drawing up a list of every way the Principal Treatment Centre could be provided in the future
- applying the fixed points and hurdle criteria to the initial list of eight possible solutions.
This resulted in our two options for the consultation:
- Evelina London Children’s Hospital which is run by Guy’s and St Thomas’ NHS Foundation Trust
and - St George’s Hospital, which is run by St George’s University Hospitals NHS Foundation Trust.
Evaluation criteria
Next, advisory and working groups and other experts advised on the development of the evaluation criteria, to help us compare and assess the two options in more detail. These covered four key areas for the future service:
- clinical services – aspects of the services the two hospitals provide that would be important for the future centre
- patient and carer experience – how the two hospitals would support children with cancer and their families
- enabling (non clinical) factors – everything the future centre would need to have to work smoothly. This included looking at the impacts on staff
- research – what the hospitals, and the Trusts that run them, do now for research and what they would offer the future centre.
They also advised on specific aspects for each of the key areas we should focus on as ‘sub-criteria’ to help us assess the two options in detail.
A lot of this was based on the national service specification for Principal Treatment Centres. Specific feedback from children, parents, staff and researchers also shaped the sub-criteria. More information on the evaluation criteria is available on our How the evaluation criteria were developed page.
The cost of the future centre is not included in the list above but is one of the hurdle criteria. This means that, so long as our work shows that both options are affordable, the cost would not influence the decision about the location of the future Principal Treatment Centre. It would be based on which option would offer the best children’s cancer service for the future. More information about the costs is available on our Finance key information at a glance page.

Identifying the most important key areas
The Programme Board discussed the key areas and how they should be scored. They weighted the most important key areas for the future Principal Treatment Centre so they would get a higher percentage of the scores. Clinical services got the highest weighting, because they were seen as the most important area.
More than 30 experts – independent nurses and doctors from London, the south east and further afield with no involvement in the current or future Principal Treatment Centre, parents, representatives of children’s cancer charities, independent researchers, managers, experts in specific fields including emergency preparedness and human resources, and staff from NHS England London and South East regions – were recruited to four panels, one for each of the key areas. Each panel, of up to 10 people with expertise in that specific area, weighted the sub-criteria for their key area.
All of this was checked by the independent Clinical Review Group in 2022. Its members discussed each of the criteria and suggested some changes, which were made. They then confirmed the criteria were suitable, comprehensive and would allow us to distinguish between the options.
The process for developing these evaluation criteria was agreed by the London Executive Team, the most senior leaders of NHS England London.
There are different views on some aspects of the criteria. More information is available on our How the evaluation criteria were developed page.
Assessing and scoring the options
The four panels – one for each key area being assessed – went on to do the assessment and scoring of the options. Travel times for parents and staff, and ongoing support for staff were rated using statistical data rather than assessed by the panels. This is usual for the NHS. However, there are different views about this approach. More information is available on our How travel times were assessed and scored for this consultation page.

The options
Information about the key areas, sub-criteria and weighting was shared with Guy’s and St Thomas’ NHS Foundation Trust, which runs Evelina London Children’s Hospital, and St George’s University Hospitals NHS Foundation Trust, which runs St George’s Hospital, before they wrote their proposals setting out how they would provide the future Principal Treatment Centre.
Overview
Both options would provide all the services that must be on the same site as the Principal Treatment Centre, including a Level 3 children’s intensive care unit.
This would:
- end hospital transfers from the specialist centre for very sick children who need or might need intensive care, eliminating the added risks and stress these transfers bring
- enable children to get more of their care on the specialist cancer ward, with fewer children admitted to the intensive care unit
- offer more services on the same site than now, reducing distress and improving experience for many children and families
- meet the national requirements and be capable of offering cutting-edge treatments that need intensive care on site.

Both would offer:
- outstanding-rated children’s healthcare and outstanding-rated education at children’s bedsides and in their hospital schools
- good facilities for parents and children, including beds for parents to stay next to their children and nearby, play specialists to support children, spaces for young children and teenagers, quiet spaces, outdoor space, parents’ rooms, a choice of cafes, self-catering options and a laundry
- the facilities needed to deliver the service and both have formally confirmed they would have the flexibility to provide the number of beds and isolation cubicles that could be needed for the future centre
- experience and expertise at supporting patients and families to deal with complex services, including at other hospitals, and through times of extreme difficulty
- plenty of experience of listening to children, young people and families and using what they say to help make services better.
These were assessed as part of the evaluation of patient and carer experience.
Neither of them:
- currently delivers the specific specialist cancer services that are based at The Royal Marsden
- would provide all services that must be readily available for the future children’s cancer centre (but which need not be on the same site).
Under both options:
- it is proposed all radiotherapy services (rather than some, as now) would be provided at University College Hospital
- neurosurgery (for brain, nervous system and spine problems) for children with cancer would continue to be at King’s College Hospital and St George’s Hospital in the same proportions as now
- tertiary (specialist) heart and kidney services needed by children with cancer would continue to be at Evelina London.
We would like to know what you think about each option and your ideas for making the change go smoothly.

Evelina London Children’s Hospital proposal
Evelina London is a purpose-built specialist children’s hospital.
In 2019/20 it treated almost 120,000 young patients living in Kent, Medway, south London, Surrey and Sussex.
All staff are experts in children’s healthcare. They have very broad and in-depth expertise and experience in children’s clinical care, including intensive care and surgery.
Evelina London is one of only four hospitals in England offering non-cancer immunotherapies (for spinal muscular atrophy).
It provides specialist heart and kidney services which gave inpatient care (mainly diagnostic tests) to 31 children in 2019/20 who were also seen at The Royal Marsden.
It provides the retrieval service which transfers acutely unwell children with cancer.
It has a children’s intensive care unit with capacity for 30 beds. Two of these beds would be expected to be needed for children with cancer.
It does not currently provide the Principal Treatment Centre or surgery to remove tumours or treat side-effects of cancer. It has a team of 54 surgeons with wide-ranging expertise and would work with them and others to create a surgical team to undertake this surgery if it became the future centre.
Evelina London works closely with the children’s neurosurgery team at King’s and funds one of their consultants.
It has more than 70 staff working on more than 180 national or international research projects in child health.
Guy’s and St Thomas NHS Foundation Trust, which runs Evelina London, attracted more than £25 million of funding for research staff in 2019/20.

If the future Principal Treatment Centre was at Evelina London, it would have:
A new children’s cancer inpatient ward in Evelina London’s main children’s hospital building. The current design features 20 beds: four cubicles suitable for bone marrow transplant patients, eight single ensuite rooms, and two bays with four beds each.
A dedicated day case unit with a procedure room in the new Children’s Day Treatment Centre and a dedicated outpatient space for children with cancer next to other facilities for children. Diagnostic services in the children’s hospital building.
Beds for parents or carers to sleep next to their child on the ward and near the children’s intensive care unit. Extra accommodation in the Ronald MacDonald House and Gassiot House.
Family friendly play areas, spaces for teenagers, and rooms for private conversations. Wifi, with a 24/7 helpline to ensure families stay connected.
Outdoor spaces on site and at a park directly opposite the hospital.
Intensive care, cancer surgery and all other expert care on site – apart from radiotherapy and services provided elsewhere which are not changing (such as specific kinds of expert care at different hospitals) including neurosurgery which would continue to be at King’s College Hospital and St George’s.
EPIC electronic health record system with King’s College Hospital. Records could be linked to The Royal Marsden, University College Hospital and Great Ormond Street Hospital. Potential for access by shared care units in local hospitals. Portal for patients and parents to use, including to communicate with clinical teams.
Research staff working alongside the teams treating children with cancer and on the two dedicated children’s research wards, the children’s intensive care unit and in dedicated children’s imaging facilities.
Access for researchers to on-site infrastructure and services including sample storage and office space at the scale and complexity essential for clinical trials. Access to Guy’s Cancer Centre for adults, including the Experimental Cancer Medicine Centre and state-of-the-art biobanking.
Guy’s and St Thomas’, which runs Evelina London, undertakes research jointly with King’s College London, which has a School of Cancer and Pharmaceutical Sciences with the Francis Crick Institute, an Institute of Cancer Policy, a School of Biomedical Engineering and Imaging Sciences. They are also part of many other partnerships including with industry.
Evelina London’s vision for children’s cancer research, if it became the future Principal Treatment Centre
It would:
- create exceptional capabilities for immunological and advanced cellular research for children’s cancer care
- develop a comprehensive clinical trial programme for children with cancer focusing on early-phase molecularly-targeted anticancer drugs
- use advanced imaging research to develop and bring into clinical trials new molecularly-targeted drugs
- develop wider research such as on how best to manage symptoms, mental health impacts of cancer, and research by nurses and allied health professionals (such as pharmacists and physios).
Extra information
Very early information from Guy’s and St Thomas’ on behalf of Evelina London described plans for the children’s cancer ward to be in another hospital building near the children’s hospital. It has since shared its intention, if Evelina London became the future Principal Treatment Centre, to locate the ward in the main children’s hospital building. The description above is based on the updated information.
St George’s Hospital proposal
St George’s is a large teaching hospital. It provides specialist services for adults and children.
In 2019/20 it treated almost 60,000 young patients mainly living in south west London, Surrey and Sussex.
All children’s services staff are experts in children’s healthcare.
It has 25 years experience of caring for children with cancer.
St George’s provides all the intensive care, most cancer surgery, four children’s cancer beds, and other specialist children’s services for the current Principal Treatment Centre, which it provides in partnership with The Royal Marsden.
It has a 14-bed children’s intensive care unit. Two of these beds, like now, would be expected to be needed for children with cancer.
It also has a children’s cancer shared care unit where children living locally can receive supportive care.
St George’s provides brain, nervous system and spinal surgery (neurosurgery), as does King’s College Hospital. In 2019/20, around 20% of children who required cancer-related neurosurgery had it at St George’s Hospital (see more information about neurosurgery above).
It has 25 children’s researchers and a good track record in national and international research.
St George’s University Hospitals NHS Foundation Trust, which runs St George’s Hospital, attracted £8.2 million of funding for research staff in 2019/20.

If the future Principal Treatment Centre was at St George’s, it would have:
A new children’s cancer centre in a converted wing of the hospital with its own entrance. The current design is for:
- 22 single ensuite rooms for children with cancer. A further six ensuite rooms would be available for use as family suites as needed (each would interconnect to one other bedroom)
- 10 of the 22 would be isolation rooms suitable for bone marrow transplant patients
- one would be a lead-lined room for specific types of treatment, if needed.
Beds for parents or carers to sleep next to their child and near the children’s intensive care unit. Extra accommodation in the Ronald McDonald House and Pelican Hotel.
Dedicated outpatient clinics and day case treatments including chemotherapy and minor operations in the cancer centre, with diagnostic services close by.
Intensive care, cancer surgery and all other expert care on site, other than services which are not changing (such as specific kinds of expert care at different hospitals), radiotherapy, and inpatient kidney and heart care, which would continue to be at Evelina London.
Dedicated research facilities in the children’s cancer centre with a laboratory and offices for staff from the Institute of Cancer Research and a clinical research unit with six clinical/consulting rooms, sample storage, a ‘hot’ laboratory and offices.
Playrooms and TV, chill out and gaming rooms for children of different ages.
Dedicated garden space which could be closed off to other patients and visitors.
Infloflex cancer management electronic patient record system. Patients can access appointment information on an app. Health Information Exchange system gives shared care units in local hospitals secure access to their patients’ records at St George’s. A portal for patients and families to use via the NHS App is being developed.
Research staff working alongside the teams treating children with cancer and on the children’s intensive care unit.
Researchers would benefit from and be supported by the hospital’s wider research infrastructure including its National Institute for Health and Care Research Clinical Research Facility and established biobank at St George’s, University of London.
St George’s collaborates on children’s cancer research and trials with the Institute of Cancer Research and The Royal Marsden, with a number of open trials at St George’s. It collaborates with St George’s, University of London. They have a joint Infection Clinical Academic Group which includes an Institute for Infection and Immunity.
St George’s Hospital’s vision for children’s cancer research, if it became the future Principal Treatment Centre
It would:
- help deliver, promote and spread children’s cancer research
- boost existing work on personalised medicine and drive forward training and commitments on early phase and other trials
- further develop research in areas such as antifungal diagnostics, convection-enhanced delivery treatment for brain tumours, optimising nutrition in children with cancer
- provide national and international opportunities for antifungal research.
What impact could the different options have?
Travel
Children and parents have a lot of questions about travel to the future children’s cancer centre. Travel times for patients and staff contributed to the scores for the two options.
Getting there
Evelina London is a few minutes’ walk away from Waterloo and Waterloo East train stations as well as London Underground stations at Lambeth North, Waterloo and Westminster.
The closest major roads are the A3 from the west and the A2 from the east.
St George’s Hospital is a few minutes walk from London Underground station Tooting Broadway and also close to Tooting train station.
The closest major roads are the A24 and the A214.
Impact on travel times
To work out the impact of the move on children and families’ travel times, an independent travel analysis looked at journey times. It was based on anonymised addresses for the patients who were admitted to hospital as inpatients in 2019/20.
The analysis found both options would be very similar or faster to get to by public transport than the current Principal Treatment Centre at The Royal Marsden and St George’s Hospital for the vast majority of people. By road, for many people going to St George’s and most going to Evelina London, it would be slower.
The table below shows the result.
| | Longer journey than to the current Principal Treatment Centre (by more than 15 minutes) | Longer journey than to the current Principal Treatment Centre (by more than 15 minutes) | Faster or very similar journey than to the current Principal Treatment Centre (no more than 15 minutes longer) | Faster or very similar journey than to the current Principal Treatment Centre (no more than 15 minutes longer) |
|---|---|---|---|---|
| Method of travel | Evelina London Children’s Hospital | St George’s Hospital | Evelina London Children’s Hospital | St George’s Hospital |
| Public transport | 6.7% | 4.6% | 93.3% | 95.4% |
| Car | 71.1% | 49.5% | 28.9% | 50.5% |
Travel times for patients living in areas which are in the 20% most deprived in the country were a key part of the scoring for the evaluation. The scoring also assumed half the patients travelled by public transport and half by road. More information on how travel times were scored is available on our how travel times were assessed and scored for this consultation page.
To understand the impact on travel times of our proposal to move conventional radiotherapy services from The Royal Marsden to University College Hospital, an independent analysis was carried out. It compared travel times to The Royal Marsden and University College Hospital by car and by public transport for all children across the catchment area.
This table shows the result.
| Method of travel | Percentage of children in the catchment area whose journey would take 60 minutes or less | Percentage of children in the catchment area whose journey would take 60 minutes or less |
|---|---|---|
| The Royal Marsden | University College Hospital | |
| Public transport | 20% | 35% |
| Car | 66% | 27% |
The analysis found University College Hospital would be faster to get to by public transport and slower by road than The Royal Marsden for most children in the catchment area.
We also looked at the impact on children living in poorer areas, and the countryside/outside London for both these proposals.
To either Evelina London or St George’s, they would have:
- shorter journeys by public transport than other children (up to 25 minutes shorter)
- longer journeys by road (up to 30 minutes longer).
To University College Hospital, children who live in poorer areas would have:
- shorter journeys by public transport than other children (up to 40 minutes shorter)
- longer journeys by road (on average 20 minutes longer).
In response to feedback, we asked current patients and parents how they get to The Royal Marsden and St George’s. Out of 88 replies:
- 81% said they travelled by car (whether their own vehicle or a taxi)
- 11% said they travelled by public transport
- 6% said they used hospital provided transport
- 1% said they travelled by bicycle
- 1% said they travelled on foot.
Concerns about how travel times were assessed and scored were raised with us. In response, we ran checks which assumed more children came by car and fewer by public transport, to see what effect that had on the scores. It reduced the scores for both options but, even if we assumed all families drove, the overall result stayed the same (see the scoring outcomes section below). More information is available on our how the options were assessed and scored page.
The group advising on our equality assessment has looked at help with travel for children and families. Both Guy’s and St Thomas’ and St George’s University Hospitals NHS Foundation Trust have been involved in this work and are committed to making things as easy as possible for children and families.
- If a child has a medical need that prevents them using public transport, they are eligible for patient transport. This would include if they are immunocompromised and have no access to a car. Patients who need to be closely monitored during the journey or are likely to need assistance because of their treatment (such as being sick) may also be eligible. Guy’s and St Thomas’, St George’s and University College Hospital have dedicated patient transport teams.
- Both Guy’s and St Thomas’ and St George’s offer parking for children and families accessing children’s cancer care. There would be a drop-off zone and dedicated parking outside the children’s cancer centre at St George’s. Through this impact assessment work, Guy’s and St Thomas’ on behalf of Evelina London, has confirmed that, in addition to an existing drop-off zone, dedicated parking for patients with weakened immune systems, including those visiting the cancer centre, would be available in the St Thomas’ Hospital car park, less than a five-minute walk away from Evelina London.
- All three organisations are able to reimburse parking and support parents of children with cancer to access reimbursement for Ultra Low Emission Zone (ULEZ) charges. Evelina London and University College Hospital could also support with reimbursement for congestion zone charges. More detail is available on TfL’s Congestion Charge and ULEZ page.
- As now, families on low income or benefits may be able to reclaim public transport costs under the Healthcare Travel Costs Scheme.
- Evelina London’s volunteers would support families as mobility assistants, especially families with disabilities. There would also be a volunteer driver scheme.
- St George’s helps families with travel arrangements for appointments and to make the journey home by taxi or patient transport after a hospital stay.
The group has also made recommendations for the future Principal Treatment Centre on how to reduce the impact of this change on families. More information can be found in the impacts of these proposed changes section above.
The Royal Marsden, in collaboration with Great Ormond Street Hospital and University College Hospital (which also provide specialist cancer services) has guidance which advises children and families that it is safe to travel on public transport for children with cancer, even with a weakened immune system.
The guidance says that for some patients it might not always be appropriate to be in crowded areas, depending on the treatment they are receiving. It says that clinicians should assess patients on a case-by-case basis.
For instance, staff at Great Ormond Street give specific advice to bone marrow transplant patients and advise, if possible not to travel at peak times.
Although hospital guidance says it is safe, parents and carers have told us they have worries about travel and would prefer to travel by car.
We are working with staff at Great Ormond Street to learn more about supporting families who need to travel to their central London location for care.

Travel times for staff
We also looked at the change in travel times for staff. The independent analysis was based on the anonymised addresses of actual members of staff at The Royal Marsden (and, for the Evelina option, St George’s) who would be able to transfer to the future centre, if they wanted to. The options appraisal looked at travel times by public transport. It found both options are very similar or faster to get to by public transport than their current workplace for most staff. The table below shows the result.
| Method of travel | Percentage of staff who would have a longer journey than to work currently (by more than 15 minutes) | Percentage of staff who would have a longer journey than to work currently (by more than 15 minutes) | Percentage of staff who would have a faster or very similar journey than to work currently (no more than 15 minutes longer) | Percentage of staff who would have a faster or very similar journey than to work currently (no more than 15 minutes longer) |
|---|---|---|---|---|
| Evelina London | St George’s | Evelina London | St George’s | |
| Public transport | 39.3% | 34.5% | 60.7% | 65.5% |
We recognise that the vast majority of staff at The Royal Marsden currently drive, walk or cycle to work and this is unlikely to be possible after the move.
We analysed average travel times for staff who drive to work at The Royal Marsden and found it is 32 minutes. Travel times to work by public transport would increase to 70 minutes to Evelina London or 69 minutes to St George’s.
To find out how St George’s staff who work for the current Principal Treatment Centre (not just those who might transfer to the new service) get to work, we asked them some questions. Of those who responded, 42% said they travel by public transport, 23% by bike, 21% by car and 14% on foot. More than half of those who replied said it takes them less than 30 minutes (10% under 15 minutes and 43% 15-30 minutes), 17% take 31-45 minutes and 20% take 46 minutes to an hour and 5% take over an hour.
Help with costs
Staff would be able to claim back extra travel costs caused by the move for up to four years, as part of their protected rights. Whichever hospital was the site of the future Principal Treatment Centre, they would also be entitled to inner London weighting.
Other NHS services
With any service change, it is important to consider its impact on other NHS services and any risks to patient care, so they can be dealt with.
Potential impact on St George’s
St George’s is concerned about the potential impact on some of its other services if the future Principal Treatment Centre was at Evelina London:
- its ability to attract and keep children’s specialist surgical staff and trainee surgeons if children’s cancer surgery (which St George’s says is about 20% of its planned operations for children) moved away, and the impact that could potentially have on the non-cancer surgery it could provide for children
- the potential impact on its children’s pathology services (which help to diagnose and guide treatment for cancer as well as many other diseases). Children’s cancer makes up a lot of the pathology team’s work and helps to attract and keep staff.
- its ability to deliver wider improvements and other benefits for non-cancer patients, including its interventional radiology service, children’s research, and improvements for specific conditions such as sickle cell disease.
It is also concerned about ongoing costs which the Trust might continue to have to pay for a while, if the service moved.
NHS England London has met with leaders from St George’s, The Royal Marsden and Evelina London to discuss these concerns. If they looked likely to become an issue, we have agreed:
- to work closely together so all patients across the area continue to get high quality care
- the importance of enabling clinicians to provide care to patients where their expertise is needed
- a commitment by NHS England to the principle of working with Trusts on reasonable costs associated with moving the services and getting them up and running, for a time.
These principles would apply to a range of other scenarios too.
Although St George’s concerns are real and reasonable, there are examples in London of excellent children’s surgery centres that do not provide cancer surgery. This shows that it is possible for a hospital to be successful without this work. New ways of working for pathology services, including having a shared workforce and managing demand differently, are already being used to make best use of available skills.

Potential impact on The Royal Marsden
NHS England will support The Royal Marsden up to and during the time when specialist children’s cancer services move to the future Principal Treatment Centre. This support includes a commitment to the principle of funding reasonable costs associated with this change for a time.
The Royal Marsden will continue to be the Principal Treatment Centre for teenage and young adult cancer services. Part of this service is currently provided by staff who support the children and young people’s service. We will work with the Trust on plans for the future.
Potential impact on Evelina London
Evelina London is concerned about a potential impact on the patient care its non-cancer specialist services could provide if the future Principal Treatment Centre was at St George’s. It believes that not being able to work with on-site specialist cancer services could make it harder for some of its staff to develop the skills needed to offer new cutting-edge treatments to children receiving non-cancer care, such as immune therapies and stem cell transplants for non-malignant conditions. If the future Principal Treatment Centre was at St George’s Hospital, Evelina London would consider how to make best use of its existing networks to share and receive learning in other ways.
Other parts of the NHS
University College Hospital is happy to work with either Trust on the proposal to provide all radiotherapy services from its site. NHS England would support transition arrangements.
We do not think these service changes would have a significant impact on services or patients in other parts of the NHS in Brighton and Hove, East Sussex, Kent, Medway, south London or Surrey.
Arrangements for how children with cancer move through NHS services would need to be carefully reviewed before the move, to make sure they still work smoothly afterwards. This would be a chance to find improvements. Patients and families would have a key role in this.
Scoring outcome
The table below shows the overall scores from our four expert panels. Guy’s and St Thomas’ NHS Foundation Trust’s proposal on behalf of Evelina London Children’s Hospital scored higher than St George’s University Hospitals NHS Foundation Trust’s proposal on behalf of St George’s Hospital (80.5% compared to 75.3%).
This information is a helpful part of the overall picture that will be considered at the end of the consultation, along with all other evidence and information that comes forward.
Overall scores
| Key areas | Evelina London | St George’s |
|---|---|---|
| 1. Clinical services | 29.6% | 27.0% |
| 2. Patient and carer experience | 20.6% | 21.8% |
| 3. Enabling (non-clinical) factors | 15.4% | 15.3% |
| 4. Research | 14.9% | 11.2% |
| Overall score | 80.5% | 75.3% |

Where the bids scored higher
Guy’s and St Thomas’ NHS Foundation Trust’s proposal on behalf of Evelina London Children’s Hospital scored higher on three of the four sub-criteria for the clinical services key area and on all three sub-criteria for research. St George’s University Hospitals NHS Foundation Trust on behalf of St George’s Hospital scored higher on two of the five sub-criteria for patient and carer experience. Other scores were the same or very similar.
The table below sets out the sub-criteria for each of the key areas and explains the scores awarded by the expert panels for each of them.
Clinical services
| Evelina London | Evelina London | Evelina London | Both hospitals |
|---|---|---|---|
| Evelina London scored higher on network effectiveness, needed for leading and coordinating children’s cancer care through the children’s cancer network. Why: It already runs children’s networks and the retrieval service for very sick children across the children’s cancer centre catchment area. The expert panel assessed that these are a good match for supporting children’s cancer care. | Evelina London scored higher for the number of the services that must be ‘readily available’ that it would have on site if it became the future Principal Treatment Centre. Why: Evelina London would have all but two of these services, while St George’s would have all but three. | Evelina London scored higher for its support for children to move on to teenage and young adult services, especially its example of how this already works for children with kidney problems. Why: its support was assessed by the panel as very good – better than the service specification. (St George’s proposal was assessed as meeting the service specification.) | Both hospitals scored the same for transfers of children to a different hospital for care. Why: they were both assessed by the panel as reducing transfers of care for children with cancer staying in their hospitals but not being able to get rid of them completely because of the way cancer services are organised in London. |
Patient and carer experience
| St George’s | St George’s | Both hospitals |
|---|---|---|
| St George’s scored higher on quality of facilities – specifically privacy and dignity. Why: St George’s proposed plans for the future centre were assessed by the expert panel as protecting patient privacy and dignity for all ages of children. | St George’s scored higher on patient travel times, especially by road. Why: A smaller number of patients would have longer travel times than now if the future centre was at St George’s rather than Evelina London. | Both hospitals scored the same for – quality of facilities, specifically education, play specialists, age-appropriateness of spaces, support for parents to stay with their child – how they would support patients’ cancer care including at other hospitals – how they would support families during times of extreme difficulty – their approach to patient and family engagement. Why: both proposals were given maximum marks by the expert panel for all these services. |
Enabling (non-clinical) factors
| Evelina London | St George’s | Both hospitals |
|---|---|---|
| Evelina London scored higher on ongoing support for staff Why: Evelina London has slightly better staff survey scores than St George’s and a lower rate of staff turnover. | St George’s scored higher on two aspects of impact on staff: – its training offer – travel times. Why – training offer: Both options scored the same on continuous professional development for staff but St George’s proposal was assessed by the expert panel to offer an enhanced package of professional training. Why – travel times: Fewer staff would have longer journeys by public transport to St George’s than to Evelina London when compared to their current journeys to work (see the staff travel times section for more information). | Both hospitals scored the same for – capacity: enough workforce, space and equipment to provide speedy access for children from across the catchment area and offer bone marrow transplants – resilience: good plans for keeping services running smoothly, including in emergencies. Why: both Trusts were assessed by the expert panel to have enough capacity to provide the future services, and strong resilience. They also both scored equally highly on benefits for staff. |
Research
| Evelina | Evelina | Evelina |
|---|---|---|
| Evelina scored higher on people, which assessed research workforce; staff development programmes; income supporting research staffing; research networks and collaboration; previous impact on collaborating to advance international health policy. | Evelina scored higher on place, which assessed current capacity and excellence – physical space for research, including infrastructure to support and enhance transferring research teams, capacity for (phase I, II, and III research) trials and tissues studies, ability to link with industry; plans to improve existing provision and capacity to scale. | Evelina scored higher on capability and performance, which assessed current research performance and capability, providers’ ambition and future vision for research and innovation. |
Why:
Evelina London was assessed by the expert panel as having the greater potential for sustaining and enhancing children’s cancer research in partnership with the Institute of Cancer Research. The reasons included:
- the strength of Evelina London’s existing children’s research and facilities
- Guy’s and St Thomas’ internationally recognised research teams and strong leadership
- the Trust’s track record including in adult cancer research (including leukaemia, stem cell transplantation and immunotherapy)
- the financial and other support it offers research-active professionals and its significant partnerships with industry.
Our preferred option
Based on the assessment by panels of experts, we have a better understanding of the strengths of both options. Both options scored highly in the pre-consultation evaluation but Evelina London Children’s Hospital scored higher. On this basis, at this stage in the process, Evelina London is the site we prefer for the future Principal Treatment Centre.
However, we are open-minded about both options and open to any other evidence that the public may share. There may also be other solutions for our case for change which we haven’t identified. We will consider any viable alternatives that are suggested.
We will only make our decision on the location of the future centre (including the proposed move of conventional radiotherapy services) after hearing the views that come forward during the public consultation and taking account of all relevant data, evidence and other factors.

Timetable and next steps
We need to hear from you
We are sharing lots of information about our proposals for the future Principal Treatment Centre, including radiotherapy services for children with cancer who live in south London and much of the south east, and the options we have identified and assessed. This is so you can have a clear understanding of what we are proposing, why, and how it would make a difference.
We really want to know your thoughts on the good points and drawbacks of each option and of our proposals for conventional radiotherapy services, as well as your ideas for making these proposed changes go smoothly. We also welcome your views, questions and any additional information you think we should know. A public consultation is not a vote or referendum. It is a chance to tell us what you think.
To have your say you can:
- complete our online questionnaire or easy read questionnaire
- register here for an online meeting on Monday 4 December
- contact us if you would like to visit Evelina London and St George’s Hospital
- invite us to a meeting you are holding
- send us an email or letter.
Phone: to leave a message, ring 0800 135 7971
Email: england.childrenscancercentre@nhs.net
By post: write to us at FREEPOST CHILDRENS CANCER CENTRE (no need for a stamp)
The decision will be taken by NHS England leaders for London and South East regions, who will consider all the feedback and additional evidence that comes forward during the consultation. It will be independently analysed and written up in a report which we will put on our website.
To shape their decision on these proposals, they will also consider all other relevant information, such as the outcome of the options evaluation process and the equality and health inequalities impact assessment. NHS England has a duty to consider how its decisions help to reach net zero carbon emissions so there will also be an environmental assessment.
So long as our work shows that both options remain affordable, the cost will not influence the decision.
Those taking the decision will:
- decide which option is taken forward and consider our proposal for conventional radiotherapy services
- identify what, if any, improvements are needed to the proposed changes and/or find solutions for any concerns.
Making it happen
Once there is final go-ahead for the future Principal Treatment Centre, we will work closely with staff in the current service, patients and their families, all the Trusts involved, the cancer network, Institute of Cancer Research, and other partners to ensure that the move to the future site, wherever it is, is as smooth as possible. All staff involved in the service will have the opportunity to be part of this work. Patients and parents will also be able to help design the new service – the team running the future centre will make sure that people from different groups and communities have the chance to get involved.
As with any change, there will be things we need to focus on managing, however, all the Trusts involved in this consultation are committed to making a success of this for children with cancer, and to working together to achieve it.

Getting information in a different language
If you or someone you know needs this consultation document in a different language, please contact us at england.childrenscancercentre@nhs.net
Dacă dumneavoastră sau cineva pe care îl cunoașteți aveți nevoie de acest document de consultare într-un alt format sau limbă, vă rugăm să ne contactați la england.childrenscancercentre@nhs.net
Si usted o alguien que conoce necesita este documento de consulta en un formato o idioma distinto, contáctenos en england.childrenscancercentre@nhs.net
Se você ou alguém que você conhece precisa deste documento de consulta num formato ou idioma diferente, entre em contato conosco atraves do england.childrenscancercentre@nhs.net
Jeśli Ty lub ktoś, kogo znasz, potrzebuje tego dokumentu konsultacyjnego w innym formacie lub języku, skontaktuj się z nami pod numerem england.childrenscancercentre@nhs.net
如果閣下或者任何人士需要另一種方式或者語言閱讀此諮詢文件,請電郵至 england.childrenscancercentre@nhs.net
i
यदि तपाईं वा तपाईंले चिन्ने व्यक्तिलाई यो परामर्श कागजात फरक ढाँचा वा भाषामा चाहिन्छ भने, कृपया हामीलाई [फोन नम्बर] वा england.childrenscancercentre@nhs.netमा सम्पर्क गर्नुहोस्।
உங்களுக்கோ அல்லது உங்களுக்குத் தெரிந்தவருக்கோ இந்த ஆலோசனை ஆவணம் வேறு வடிவத்தில் அல்லது மொழியில் தேவைப்பட்டால், எங்களை [தொலைபேசி எண்] அல்லது england.childrenscancercentre@nhs.netஇல் தொடர்பு கொள்ளவும்.
Siz veya tanıdığınız birinin bu danışma belgesinin farklı bir formatta veya dilde olması gerekiyorsa, lütfen england.childrenscancercentre@nhs.net adresinden bizimle iletişime geçin.
Acknowledgements
We are very grateful for the assistance from the teams at Evelina London, St George’s Hospital and The Royal Marsden with preparation of this document. We are also grateful for images provided by Evelina London, St George’s Hospital and Young Lives Vs Cancer/Barry Willis Photography, with the families’ kind permission.
This information was produced by NHS England in September 2023 with support from Transformation Partners in Health and Care, and updated in October 2023.
