This page is no longer being updated from 31st March 2025.
Please visit Evelina London’s website here to view information and how to get involved.
Introduction
The following information explains how we arrived at the two options for the future Principal Treatment Centre that we are consulting on. These options are:
- Evelina London Children’s Hospital, Lambeth, south London, with conventional radiotherapy services provided at University College Hospital
and
- St George’s Hospital, Tooting, south London, with conventional radiotherapy services provided at University College Hospital
1. Setting up the programme
NHS England London, which plans and pays for specialised services based in London for children with cancer, was tasked by the national NHS England Board with identifying and commissioning a future Principal Treatment Centre which is compliant with the national service specification for Principal Treatment Centres for children’s cancer.
This followed the national board’s acceptance of Professor Sir Mike Richards’ report in January 2020 and its finding that all Principal Treatment Centres for children’s cancer funded by NHS England must be on the same site as a Level 3 children’s intensive care unit.
In response, NHS England London (working in partnership with NHS England South East) set up the South London and South East Principal Treatment Centre Programme to identify an affordable, clinically viable and deliverable option for the future Principal Treatment Centre on the same site as a Level 3 children’s intensive care unit.
2. How the programme works
The programme is overseen by a Programme Board which is made up of leaders from the hospitals involved, senior doctors from NHS England London and NHS England South East, and external experts. It is supported by clinical, managerial, finance and patient voice advisory groups. It started work in July 2020.
The aim of the programme is to commission the best possible Principal Treatment Centre for children with cancer in Brighton and Hove, East Sussex, Kent, Medway, south London and most of Surrey – the catchment area.
The day-to-day work of the programme is led by the NHS England London specialised commissioning team in partnership with NHS England South East.
3. Process it is following
A formal reconfiguration process is required when proposing to move a significant service from one site to another to ensure all stakeholders have the opportunity to review, comment on and help shape the case for change, clinical model and proposals [1]. [1] NHS England » Planning, assuring and delivering service change for patients
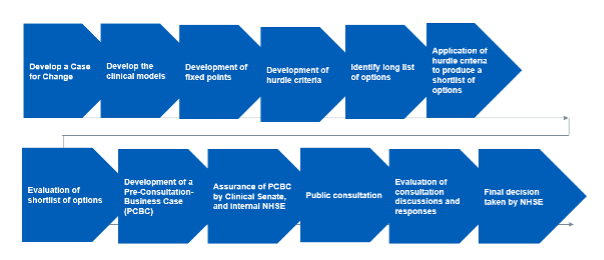
The programme is following NHS England guidance and the standard NHS process for reconfiguring services which is summarised in the diagram below.
Step 1: develop a case for change
There are five main reasons for our proposed changes to the very specialist cancer treatment services for children provided at The Royal Marsden for children with cancer who live in south London and much of the south east.
- The current Principal Treatment Centre does not meet national service specification requirements
- Hospital transfers of very sick children for intensive care add risks and stress
- The intensive care team is not currently able to provide face-to-face advice on the care of children on the ward
- There is a need to improve children and families’ experience when patients require intensive care and other specialist children’s services
- Although it offers a wide range of innovative treatments, the current Principal Treatment Centre is excluded from giving a specific type of new treatment, and others expected in the future
Step 2: develop the clinical models
Principal Treatment Centres for children with cancer are responsible for making sure each child gets the specific expert care they need. Their clinical teams diagnose illness, draw up treatment plans, give specialist care, and coordinate treatment for all children aged 15 and under with cancer in their catchment area (and occasionally, older children, depending on their needs). They work with other cancer services including shared care units in more local hospitals (which are not affected by this consultation).
Our clinical model is to provide children’s cancer services that are fully compliant with the national service specification published in November 2021 [1]. The national service specification for Principal Treatment Centres for children’s cancer set the clinical model; it is our responsibility to see that it is implemented. For the Principal Treatment Centre for children with cancer who live in south London and much of the south east, this will mean a reconfiguration of services. In implementing the new Principal Treatment Centre service specification, there is a significant opportunity to build on the current very good services to create a children’s cancer centre in south London that can deliver best quality care and achieve world class outcomes for children with cancer that are maintained for decades to come, while supporting a vibrant network of shared care units based in hospitals across the catchment area, increasing the support for children to be cared for closer to home.
[1] NHS England » Children’s cancer services: Principal treatment centres service specification
Step 3: develop fixed points
Fixed points in a reconfiguration programme are those agreed elements which will not change as a result of the service reconfiguration. The fixed points for this programme and the reasoning behind them were agreed by the Programme Board in November 2020, these were:
a, it is a fixed point that the proposed options must deliver a Principal Treatment Centre on the same site as a paediatric intensive care unit.
This is the purpose of the programme. Its success must not depend on changes to other models of care.
b, delivery of the programme must not be dependent on changes to other models of care that are outside the scope of this process, it is [therefore] a fixed point that activity at the following sites is not required to move as part of this reconfiguration:
- bone tumour (sarcoma) surgery at Royal National Orthopaedic Hospital, Stanmore
- brain, spinal and nervous system surgery (neurosurgery) at King’s College Hospital (King’s) and St George’s Hospital
- care of under one-year-olds with cancer of any type at Great Ormond Street Hospital
- children’s eye tumour (retinoblastoma) surgery at the Royal London Hospital
- children’s liver surgery at King’s existing paediatric intensive care units in south London at Evelina London Children’s Hospital, King’s and St George’s Hospital
- proton beam therapy and other superspecialist forms of radiotherapy at University College London Hospitals.
c, it is a fixed point that the future Principal Treatment Centre for south London and much of the south east should not be wholly located in north London
The services being configured are for patients in south London and much of the south east and should not introduce unreasonable geographic inequalities.
d, it is a fixed point that Great Ormond Street Hospital for Children NHS Foundation Trust (GOSH) working with University College London Hospitals NHS Foundation Trust (UCLH) remains the Principal Treatment Centre for north London.
GOSH/UCLH currently provides the Principal Treatment Centre for children living in north London and the surrounding geography. The national service specification has required a refresh of their roles. Once this work is completed, all Principal Treatment Centre services for children under 13 from this catchment area will be at GOSH, complemented by an enhanced level B paediatric oncology shared care unit for children under 13 at UCLH. GOSH will provide the Principal Treatment Centre for children aged 13 to 15 jointly with UCLH.
Step 4: develop hurdle criteria
Hurdle criteria are to make sure that options which are evaluated further are capable of delivering the objectives of the future service. An option on the long list either does or doesn’t meet the hurdle criteria. If it doesn’t, then it does not get carried forward to the shortlist of options. The hurdle criteria, agreed by the Programme Board in November 2020, were:
- access: the future Principal Treatment Centre must be accessible in terms of journey time for people across the catchment area and should therefore be based within Greater London
- supplier capability: to deliver the future Principal Treatment Centre, the Trust must be capable of providing a Level 3 paediatric intensive care unit which complies with the NHS England service specification (PDF) for Level 3 paediatric intensive care units and the ‘must do’ requirements in the Principal Treatment Centre specification.
- achievability: to be considered as a potential option for the future Principal Treatment Centre, provider Trusts must be willingto participate in providing the service. This was assessed by requesting providers sponsoring a solution on the long list to formally confirm an expression of interest in providing the service.
A fourth hurdle criterion was added following discussion of the evaluation criteria at the December 2020 Programme Board:
- ability to deliver the future principal treatment centre within a 2.5 year implementation timeline following final go-ahead. This timescale was considered feasible, reflecting the need to transfer the service in a timely way, yet with sufficient time for careful planning alongside relevant approvals, such as those for capital and associated estates work.
A fifth hurdle criterion was added at the March 2022 meeting of the Programme Board:
- capital and revenue affordability and deliverability tests are met: NHS England has laid out the process to follow for service changes in ‘Planning, Assuring and Delivering Service Change for Patients 2018’. The key financial test is that any proposal is affordable in capital and revenue terms ahead of public consultation. This is the approach NHS England London has used to evaluate the financial content of proposals.
The Trusts which want to provide the future centre must show that they can afford both the capital and revenue costs included in their proposals in line with existing commissioner allocations and nationally available capital.
So long as both options remain affordable, finance will not be the determining factor. Instead, we are focusing on which site can best provide what we are looking for: a future Principal Treatment Centre that gives best quality care and achieves world class outcomes for children with cancer that are maintained for decades to come.
In May 2022, the national team confirmed that £20 million of national capital would be available as a contribution toward the capital costs of the future Principal Treatment Centre.
Step 5: develop the long list
NHS England London’s public health team undertook a background review of other Principal Treatment Centres, drawing on experience in England but also looking at the service in the Netherlands where there is one large central expert centre for the country. They then drew up a list of every possible way the Principal Treatment Centre could be provided in the future. It listed eight different possible solutions (the long list). These are set out below.
Step 6: Application of fixed points and hurdle criteria to create a shortlist of options
The fixed points and hurdle criteria were applied to the long list in early 2021, resulting in an initial short list of three possible solutions, two of which would involve The Royal Marsden. In November 2021, the national service specification for Principal Treatment Centres for children’s cancer was published. The Royal Marsden confirmed it would not be able to provide a children’s intensive care unit at the Sutton site because that would not be clinically or financially sustainable. (Children’s intensive care units are always on sites used by many thousands of children every year because intensive care teams need to see tens of thousands of very sick children to maintain their specialist skills and expertise. This wouldn’t be supported by the number of children at The Royal Marsden.)
As a result, the fixed points and hurdle criteria were applied again. This resulted in the following assessment with only one possible solution – highlighted in green in the table below – met all the criteria.
4. The result of applying the fixed points and hurdle criteria
| Possible solutions identified for the Principal Treatment Centre for children with cancer living in Brighton and Hove, East Sussex, Kent, Medway, south London, and most of Surrey | How each solution measures up against the fixed points and hurdle criteria | Result |
|---|---|---|
| 1. Do nothing | The current service doesn’t comply with the ‘supplier capability’ hurdle: to deliver a service that is compliant with the national service specification. Nor does it meet fixed point (a): the future service must be on the same site as a paediatric intensive care unit. It is therefore not possible ‘to do nothing.’ | [icon name=”xmark” prefix=”fas”] |
| 2. New site developed for a standalone Principal Treatment Centre which does not currently have a paediatric intensive care unit or significant specialist services. Greenfield or district general hospital (including the current Sutton site). | Does not comply with the ‘supplier capability’ hurdle or fixed point (b) in that a new paediatric intensive care unit would not be sustainable on a new site without destabilising existing paediatric intensive care units. | [icon name=”xmark” prefix=”fas”] |
| 3. A single Principal Treatment Centre for London based on the existing compliant Principal Treatment Centre (provided by GOSH/UCLH). | Doesn’t comply with fixed point (c) in that the future Principal Treatment Centre for south London and much of the south east must not be wholly located in north London. | [icon name=”xmark” prefix=”fas”] |
| 4. Single Principal Treatment Centre for London delivered through a combination of providers based on the existing compliant Principal Treatment Centre and a second site with significant specialist services. | Various ways of delivering this were considered: GOSH/UCLH and a north London site – this combination does not comply with fixed point (c) that the future Principal Treatment Centre for south London and much of the south east must not be wholly located in north London. GOSH/UCLH with a south London partner – this combination does not comply with the ‘service capability’ hurdle as both sites would need to have intensive care units, or with the ‘achievability’ hurdle. The Royal Marsden was the only Trust wishing to partner with GOSH to deliver a Principal Treatment Centre and The Royal Marsden does not have a paediatric intensive care unit. | [icon name=”xmark” prefix=”fas”] |
| 5. A Principal Treatment Centre at an existing specialist paediatric provider in south London which has a co-located paediatric intensive care unit and all the specialist children’s services that must be delivered on site at every Principal Treatment Centre | Passes all fixed points and hurdle criteria – the only potential solution to do so. | [icon name=”check” prefix=”fas”] |
| 6. Joint site Principal Treatment Centre in the south east and south London catchment area | Doesn’t comply with the ‘supplier capability’ or ‘achievability’ hurdles as there was no combination of willing providers which put forward a compliant option. A solution including The Royal Marsden would not deliver a compliant service. | [icon name=”xmark” prefix=”fas”] |
| 7. Second Principal Treatment Centre site in the area covered by the GOSH/UCLH Principal Treatment Centre | Doesn’t comply with fixed point (c) in that the future Principal Treatment Centre for south London and much of the south east must not be wholly based in north London. | [icon name=”xmark” prefix=”fas”] |
| 8. Second Principal Treatment Centre site, in the Principal Treatment Centre catchment area but outside London. | Doesn’t comply with hurdle criteria on ‘access’ – the site must be within London for access reasons. | [icon name=”xmark” prefix=”fas”] |
This process identified that the only viable solution to deliver the service specification is a Principal Treatment Centre at an existing specialist paediatric provider in south London with a paediatric intensive care unit on site, and all the specialist children’s services that must be delivered on site at every Principal Treatment Centre (as per the service specification).
There are three Trusts which could potentially deliver the Principal Treatment Centre, because they meet all the criteria:
- Guy’s and St Thomas’ NHS Foundation Trust which runs Evelina London Children’s Hospital
- King’s College Hospital NHS Foundation Trust which runs King’s College Hospital
- St George’s University Hospitals NHS Foundation Trust which runs St George’s Hospital.
All three were written to, to ask whether they believed they still met the hurdle criteria and would be willing to continue with the process.
King’s indicated it did not want to be considered and was excluded based on the third hurdle criterion, ‘achievability’. This left the two options which we propose consulting on:
- Guy’s and St Thomas’ NHS Foundation Trust which runs Evelina London Children’s Hospital
- St George’s University Hospitals NHS Foundation Trust which runs St George’s Hospital.
As part of the current Principal Treatment Centre, The Royal Marsden is working closely and constructively with NHS England, its patients and families, and its staff to contribute to the review process. The Board of the Royal Marsden NHS Foundation Trust acknowledges that the decision on mandatory co-location of a Principal Treatment Centre with a paediatric intensive care unit has been taken by the NHS England Board. It has made clear that, in the context of this change in the service specification, it will contribute actively to the review process to ensure the very best outcome is achieved for children and families, including making the changes that may be required to respond to the development of new technologies and treatments. It has set out this position in a letter to NHS England.
5. Two potential options for the future Principal Treatment Centre
There are two options for achieving compliance with the service specification once the fixed points and hurdle criteria have been applied to the original long list. The options available for the establishment of a compliant Principal Treatment Centre for south London and much of the south east are either:
- Evelina London Children’s Hospital (Evelina London) which is part of Guy’s and St Thomas’ NHS Foundation Trust (Guy’s and St Thomas’)
or
- St George’s Hospital which is part of St George’s University Hospitals NHS Foundation Trust (St George’s) and also part of St George’s, Epsom and St Helier Hospitals and Health Group.
If Evelina London became the future Principal Treatment Centre, it would have all the specialist children’s cancer services currently at The Royal Marsden (except conventional radiotherapy) and the specialist children’s cancer services currently provided for the Principal Treatment Centre at St George’s alongside its well-established children’s intensive care unit and other specialist children’s services.
If St George’s became the future Principal Treatment Centre, it would have all the specialist children’s cancer services currently at The Royal Marsden (except conventional radiotherapy) alongside its well-established children’s intensive care unit and other specialist children’s services, including the services it already provides for the Principal Treatment Centre.
Under both options, St George’s would continue to provide a children’s cancer shared unit for local children, and its neurosurgery services. We propose that, under both options, all radiotherapy services would be provided by University College Hospital (part of University College London Hospitals NHS Foundation Trust). Children would continue to travel for some specialist cancer services because of the specific expertise hospitals have in these areas.
The consultation will help the senior leaders for NHS England (London and South East regions):
- decide which option is taken forward
- identify what, if any, improvements are needed to the proposed changes and/or find solutions for any concerns.
To do that, they will consider all the feedback and additional evidence that comes forward during the consultation. It will be analysed by an external organisation and written up in a report which we will put on our website.
They will also consider all other relevant information, such as the outcome of the options evaluation process, and the equality and health inequalities impact assessment.